Reader response and some brief news updates you can use
Myron Yaster MD

In the recent PAAD on cognitive errors in the OR here I (MY) recounted that early in my career, succinylcholine was distributed in square bottles to prevent look-alike medication errors. I asked Amanda Helfers of the Wood library for pictures to show you.
From Amanda Helfers, WLM Museum Specialist, It was more than just square bottles! Another mage from the Wood Library-Museum of Anesthesiology succinylcholine (Anectine)
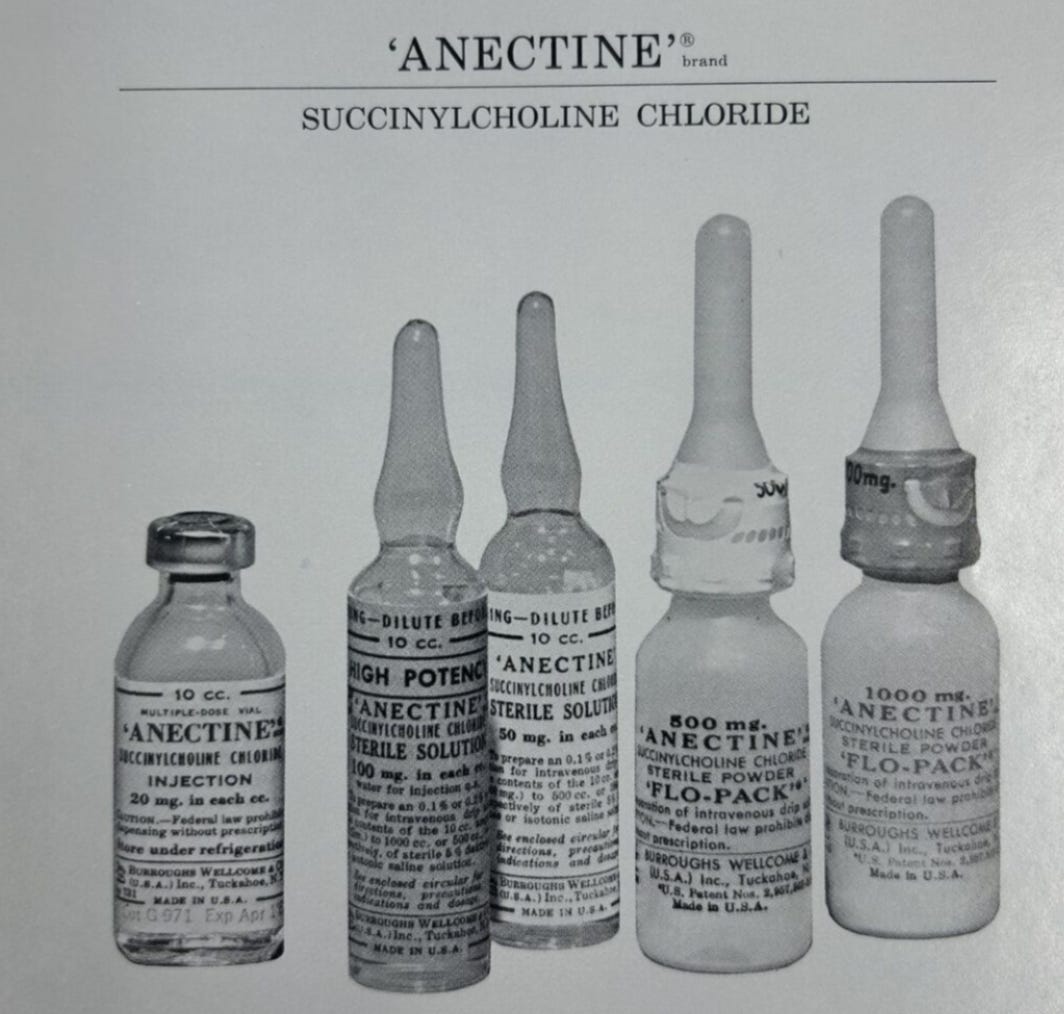
Notice in this image, the bottle of succinylcholine (Anectine) on the left is dispensed in a square bottle. Additionally, notice the 2 “flow pack” bottles on the right. This was succinylcholine in a powder form (500 or 1,000 mg) that could be diluted in saline and administered by continuous infusion for prolonged (and controllable) paralysis.
From Alexandra Donaldson MBBS FANZCA, Senior Staff Specialist Queensland Children’s Hospital
I am an Anaesthetist in Brisbane, Queensland, Australia. I work in both adult and paediatric practice, and a mix of public and private work places. I am a regular reader of the PAAD, and was interested to read the article and editorial on Communication skills here. I have a particular interest in this area of our practice and was keen to share some additional information and resources with you and the PAAD readers.
In my role as a staff specialist at the Queensland Children’s Hospital, I lead the Perioperative anxiety clinic, as well as a program called CALM Care (Comfort Analgesia Language Mindfulness Memory) which aims to provide support for all medical procedural care, to reduce potential pain and distress.
The Perioperative Anxiety clinic supports children who require more considered planning for anaesthesia via either pharmacological, or non pharmacological modifications.
I also am a founding co chair and remain on the subcommittee for EPIC - (Effective Peri-procedural Communication) group from SPANZA (Society for Paeds Anaesthetists Australia and New Zealand) (https://epickids.org.au/ )
A big focus of all this work is the importance of language, the words we choose to use, as well as the non verbal skills to support rapport building and discussion in pre op consult, and at anaesthetic induction. All with the aim to reduce anxiety, and the possible short and longer term complications we know can occur with distress and anxiety prior to anaesthesia and in particular at induction.
Through EPIC, we run courses for all health care professionals who support children having procedural care. The focus is upon the importance of communication skills and as well as teaching imaginative techniques, (similar to hypnosis skills), to support children and their caregivers at the time of procedural care. The websites have resources for all involved in the episode of care. Caregivers to support their understanding of how to prepare children for procedural care. Resources for children themselves, as well as the health professionals who look after them.
I am very happy to share any additional information or background about these models of care, courses and resources.

From Jonathan D Blank MD commenting on It’s Not Your Fault-Or Is It? The Cognitive Basis for Errors here
The concept of cognition and errors is very important and serious undertaking by every anesthesiologist involved in patient care. And it is in coming to “be educated and work harder at the situation of confirming drug appropriate, and dosing care. However, any point of care events besides having pre-filled syringes in the operating room setting versus on the floor or in the ICU only leads to a severe or significant delay in medical care. Any patient any person who has been witnessed to ICU point of care, pain control point of care, multiple checks, verbal, and computer based can test to the fact that pain care medication care is delayed and has a massive human time overage. To insist that the operating room would go to any type of point of care that isn’t excessively automatic in the checking which at this point in time there is no system that can give a verbal response as you pull a drug that’s in your hand as you’re connecting to the patient there have been in the past Are report of pharmacist doing this type of work and standing in the operating room to review medication doses with the physicians. To that article, I responded that pharmacist distribute medications. They do not give medication and to have some physician in an operating room having his handheld or his consciousness held by a pharmacist doing a one by one review. I’m not sure why I went to medical school.
I hope that the professionals that go into Anesthesia and Anesthesia Care always keep their heads above Water recessive situation on a constant basis and or cognizant of the risk however, I don’t think in the human system that you can take it away unless you as you note in your articles, spend the tremendous amount of money to make it very AI based and not consuming.
From Laurentiu Lupu MD Laurentiu Lupu MD on Remembering Karen Ann Quinlan: The case that sparked the movement for patients’ rights near the end of life here
What still feels so powerful about Quinlan is that it did more than move authority from physicians to families. It dissolved a hiding place.
Before cases like this, the medical imagination could treat the continuation of treatment as the safest ethical ground, because stopping felt like an act while continuing felt like neutrality, as if disease, not the clinician, were the agent, and the physician were merely declining to interfere. Quinlan exposed that as an illusion. Continuing a life-sustaining intervention is also a choice, with its own moral weight, its own implicit interpretation of the person, and its own cost to the family made to watch a body preserved after the life they recognized had become unreachable.
The case is remembered for expanding patient rights, but it did something quieter and just as radical: it abolished the default that had let everyone avoid authorship. Afterward, both continuing and stopping were decisions someone had to own.
This is why surrogate decision-making is more than a legal mechanism. The standard the court reached for was not the surrogate’s preference but the patient’s, what this person would have wanted. The task is therefore paradoxical: to keep a silenced person’s voice authoritative at the very moment they cannot raise it.
And the difficulty is that the body has not gone silent at all. It breathes, it persists, it goes on producing the loudest signal in the room. The surrogate’s real work is to keep that signal from being mistaken for the person’s will, to protect the patient from being reduced to physiology exactly when they can no longer speak against the reduction.
The hard lesson stays current: medicine must preserve life without letting life-preservation become an automatic moral reflex. Sometimes respecting the patient means recognizing that the most aggressive form of treatment can be the least faithful form of care.
From Dr Nick Marsden BSc MBBS FRCA MSc FANZCA, Consultant Anaesthetist, Perth Children’s Hospital
I read your post with great interest. I think the reference to Daniel Kahneman’s work, although attractive, should be treated with a degree of skepticism (especially in healthcare). To say that the human brain has two modes of thinking is an oversimplification, that suggests that the brain is a rational, algorithmic/mathematical object. Our brains are not in a constant state of flux between fast and slow thinking, it is far more complex than that, and if patient safety is to get anywhere, we should acknowledge the complexity of thought, decision making and the impact that the environment and human relations has on these processes. There is an interesting concept from Erik Hollnagel, which I think makes more sense to how healthcare operates. This is called the Efficiency Thoroughness Trade Off (ETTO), where there is recognition that to get the job done is often in conflict with environments, workflows, processes and procedures that dictate how the job should be done (1) . How we think is not as important as how we are FORCED to think by the situation in front of us. Perhaps these can be ‘designed out’, but every new concept comes with balancing measures and will likely require ongoing design, not single interventions. This is where Quality Improvement (may) help, but this requires time, money and significant effort. Where we might be careful is the idea that automation can reduce errors/incidents, as this is a concept initially borrowed from industry (The Ford Motor Company) that primarily aimed to increase productivity and profit (2). The ‘logisitical barriers’ that are mentioned may be that the processes of simplification/automation have not been shown to reduce errors (although how to demonstrate this seems to me an impossibility). Forcing functions e.g. EMR alerts are easily ignored and suffer alert fatigue (a concept you covered recently). Drug labelling still requires levels of checking and can still be bypassed (3). So, what is to be done? We are both the problem and the solution concurrently it seems. ‘Try harder’ doesn’t work, education doesn’t work, blame and shame DEFINITELY doesn’t work (but is a useful deflection). Martin Bromiley (husband of the late Elaine Bromiley, if unfamiliar then I urge you to look up the case) wrote: As clinicians the world over have reviewed my late wife’s case, in a quiet break room perhaps, they have all, with very few exceptions stated clearly: “I wouldn’t have done what they did”. Yet place those same people in a simulated scenario with the same real world disorder, most actually do (4). Automating processes might help, but it may make actually doing the work impossible, as automation can be thought of as rules based or ‘work as prescribed’ work. When we align ‘work as prescribed’ fully with ‘work as done’ we end up with what British Rail in the 1960’s United Kingdom became familiar with which is ‘work to rule’, a form of industrial action, where total following of the rules results in a shutdown of actual work (5). I agree with the notion that Anaesthetists are a powerful voice, but then I ask the author, what do they think we have been doing all this time? Anaesthetists have always advocated, and sometimes lead patient safety, because we recognise the hazards inherent to our work. The fact that errors occur is not the result of inaction, but of action (doing a high-risk job). We know that anaesthesia is very safe, but is it getting safer e.g. errors are reducing? So far none of us know the answer.
Marshall, M. W. (1957). “Automation” Today and in 1662. American Speech, 32(2), 149–151. https://doi.org/10.2307/453032
https://skybrary.aero/sites/default/files/bookshelf/3948.pdf
http://news.bbc.co.uk/onthisday/hi/dates/stories/june/24/newsid_2943000/2943686.stm
Max Feinstein Videos
Dr. Max M. Feinstein is a pediatric cardiac anesthesiologist and an Assistant Professor of Anesthesiology practicing in the Department of Anesthesiology at the Columbia University Medical Center, New York City. He runs an educational YouTube channel that aims to increase understanding about the role of anesthesiologists in healthcare: Here are 2 recent ones that were sent to Myron for the PAAD readership.
From Variety
Disney, Philips Launch Themed MRI Machines Using ‘Beloved Stories and Characters’ to Comfort Children Undergoing Scans
Disney has collaborated with Dutch health-tech multinational Philips to create themed MRI scanners for children undergoing imaging procedures.
The scanners, which launched this week in the U.S. and U.K. among a handful of other countries, will see Disney stories and characters integrated into Philips Ambient Experience for MRI to create an immersive environment resulting in a more calming experience for patients.
From CDC Morbidity and Mortality Weekly report
Characteristics of Patients Hospitalized with Measles During an Outbreak — West Texas, January–March 2025 Weekly / May 28, 2026 / 75(20);252–257
https://www.cdc.gov/mmwr/volumes/75/wr/mm7520a1.htm?s_cid=OS_mm7520a1_w
During the first two months of a large measles outbreak in West Texas (January–March 2025), 325 confirmed cases resulted in 60 hospitalizations and one measles-associated death. Among 54 hospitalized patients with available medical records, most were unvaccinated children, particularly those younger than five years. Complications were common, occurring in 87% of hospitalized patients, with pneumonia (72%), dehydration (46%), and diarrhea (39%) predominating. Four patients required intensive care, and more than 70% received supplemental oxygen. Notably, four of five hospitalized adults were pregnant women, and two infants born during maternal hospitalization developed neonatal measles. The findings underscore the substantial morbidity associated with measles and reinforce the critical importance of timely MMR vaccination to prevent severe disease, hospitalization, and outbreak-related complications.
From New England J of Medicine
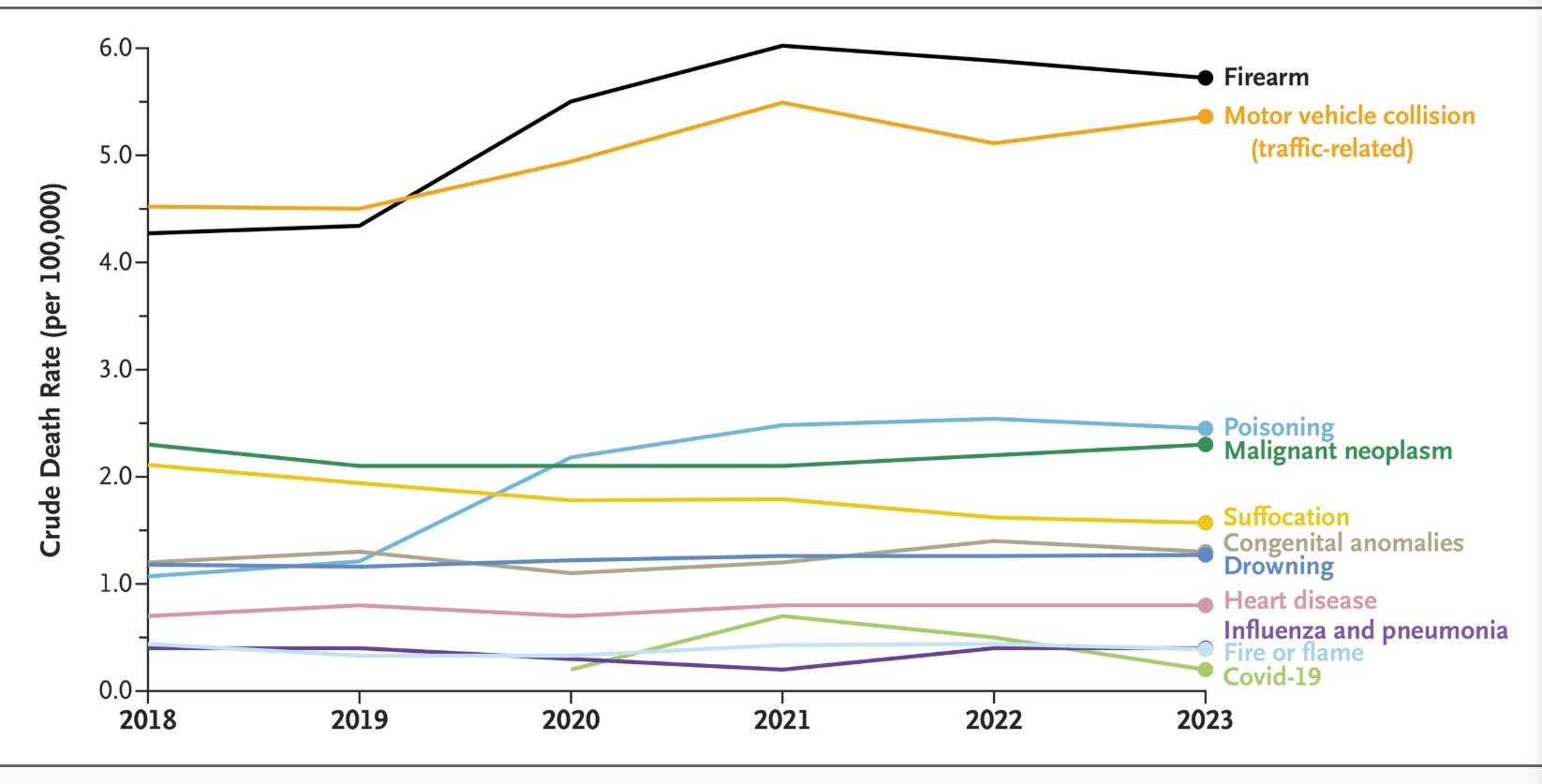
Raymond-King C, Jeffery MM, Melnick ER. Current Causes of Death among Children and Adolescents in the United States. N Engl J Med. 2026 May 14;394(19):1958-1959. doi: 10.1056/NEJMc2600445. PMID: 42127398.
From 2020 through 2023, the overall crude rate of death among children and adolescents increased by 6.6%. In 2023, a total of 22,841 children and adolescents died in the United States, and among the leading causes of death, seven are commonly encountered as sudden, life-threatening events in children or adolescents who are admitted to an emergency department. These events include firearm-related injury, motor vehicle collision, poisoning, suffocation, drowning, fire-related injury, and influenza and pneumonia