
Risk Without Terror in Anesthesia Consent
Myron Yaster MD, Lynne G. Maxwell MD, Genie Heitmiller MD

For those of you who know me, I (MY) am way outside the bell-shaped curve on the issue of anesthesia informed consent. I never really understood or believed that formal written informed consent for anesthesia before a surgical procedure was necessary or even valid. If a parent or patient gave consent for surgery, in reality they are also giving consent for anesthesia. Indeed, what is the alternative? Surgery without anesthesia? Further, in 2026, the risk of an anesthesia death, the most feared outcome, in an ASA 1-3 patient is in the 1:250,000 range…meaning that the drive to the hospital was a greater risk than the anesthetic. I always thought that the anesthesia and surgical experience for patients and their families were scary enough. Warning of potential death from anesthesia, a common theme in the consent process, was simply counter productive, unnecessary and would produce nocebo effects.
As a resident, I (LGM) had a consciousness-raising experience similar to that described by Dr. Dutton in his editorial. I was speaking about the anesthesia plan, risks and safety with a 75 year old frail woman prior to her having a laryngectomy for cancer. She was very anxious but was listening carefully to me, asking good questions. I was interrupted by the arrival of her surgeon who stood at the end of her stretcher and recited the surgical plan in a monotone, not allowing her to ask questions or respond in any way:
After you are asleep we will take the cancer out. We will do a tracheotomy and when you wake up there will be a tube in your neck that you will breathe through. There will be a tube in your nose that you will be fed through.
After he walked away, the patient was tearful and trembling. It was clear that she was unable to further process what I was telling her about the anesthesia plan for keeping her safe. Seeing the level of her anxiety and the fact that she was also fearful of the preoperative IV placement, I thought of what we had started doing in pediatric patients – administering a dose of IV midazolam mixed with Tylenol solution, given orally to reduce her anxiety and make IV placement easier. Although the adult preop nurses were skeptical that this was permissible, I was allowed to proceed. Within 15 minutes of taking the midazolam/Tylenol mixture, the patient was calmer and even smiling, and had an uneventful IV placement and anesthesia induction. Of all Dr. Dutton’s recommendations, I learned that sitting down rather than standing, looming over the patient, as the surgeon had done, was key to connecting and informing/reassuring the patient.
We’ve discussed anesthesia consent in a recent PAAD here which elicited a lot of reader responses here. In today’s PAAD, Zech et al.1 and its accompanying editorial by Dutton2 take another look at the interview and consent process. I would urge you to read these articles in their entirety, particularly Dr. Dutton’s editorial, discuss them in the OR and your faculty meetings and visit Dr. Dutton’s United States Anesthesia Partners (USAP) website https://online.usap.com/USAPPatientGuide/ ), which after I viewed it, think is a fantastic resource. I (MY) should add that Dr. Dutton is the Chief Quality Officer of USAP and I worked with him early in his career at Johns Hopkins and the University of Maryland.
Original article
Zech N, Bauer A, Hansen E. Communication Training for the Preoperative Anesthesia Consultation Reduces Anxiety: A Prospective, Patient-Blinded Pre-Post Intervention Study. Anesth Analg. 2026 May 1;142(5):869-878. doi: 10.1213/ANE.0000000000007791. Epub 2026 Apr 14. PMID: 41342609.
Editorial
Dutton RP. Risk Without Terror in Anesthesia Consent. Anesth Analg. 2026 May 1;142(5):866-868. doi: 10.1213/ANE.0000000000007865. Epub 2025 Nov 24. PMID: 41285000.
Because we work in the hospital or ambulatory surgery center every day, we often forget just how terrifying an experience it is for our pediatric patients and their families. We dress in different clothing (scrubs) and wear masks. Our patients have been fasted, are hungry and thirsty, their parents are usually frightened and won’t feed them, and there is a distinct smell of antiseptic cleaning solutions in the air. We often magnify the terror during the interview and consent process when we discuss in graphic detail what’s going to happen and discuss the possible negative complications including death.
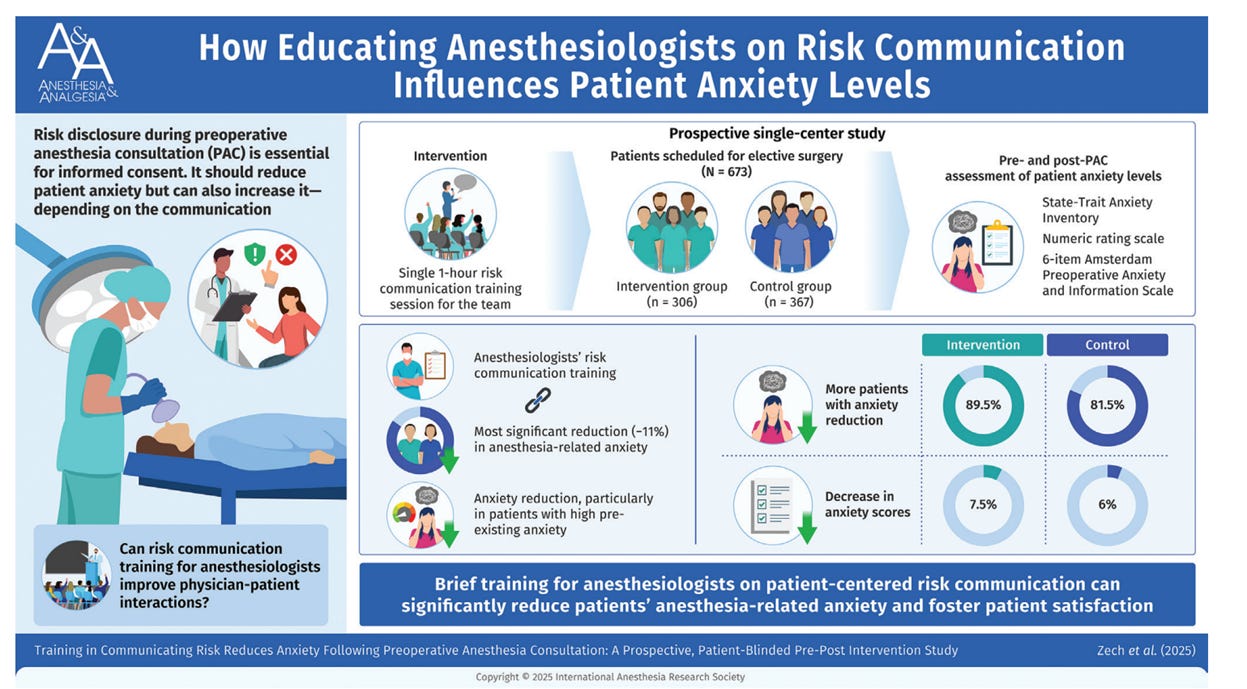
Zech et al.’s “goal was to help clinicians communicate necessary preoperative information while emphasizing the positive benefits of the procedure, the comprehensive nature of anesthesia monitoring, and the prophylactic mitigation of pain and nausea. The study itself was a structured assessment of ADULT patient anxiety before and after the preoperative interview, stratified by whether the anesthetist had undergone the research team’s novel 1-hour training on effective communication.”1,2
This single-center study enrolled 673 adult patients undergoing elective surgery, comparing outcomes between a control group (n=367) and an intervention group (n=306). The intervention consisted of a single 1-hour communication training session for anesthesiologists, focused on patient-centered risk communication strategies. These included positive framing of risk information, avoidance of negations, contextualization of risk frequencies, identification and neutralization of preexisting negative expectations, and simultaneous emphasis on treatment benefits, monitoring, and safety. Importantly, the intervention did not reduce the extent of risk disclosure but modified its delivery to minimize nocebo effects.
Patient anxiety was assessed immediately before and after the PAC using three validated instruments: the State-Trait Anxiety Inventory (STAI-S), the Amsterdam Preoperative Anxiety and Information Scale (APAIS), and a numeric rating scale (NRS). Baseline anxiety levels were substantial, with a mean STAI-S score of 41.6 ± 11.7 and 47% of patients exhibiting clinically significant anxiety (STAI-S >40). Surgery-related anxiety exceeded anesthesia-related anxiety at baseline (APAIS 5.0 ± 2.2 vs 3.5 ± 1.6, respectively).
OK, what did they find? The primary finding was that communication training significantly enhanced anxiety reduction. In the intervention group, 89.5% of patients experienced decreased anxiety compared with 81.5% in the control group (p=0.003). Patients with high baseline anxiety derived the greatest benefit from the intervention. Among individuals with STAI-S scores > 40, the reduction in anxiety was significantly greater in the intervention group (ΔSTAI-S −4.9 ± 6.4 vs −3.3 ± 6.6; p=0.033). This finding highlights the potential for targeted communication strategies to improve outcomes in vulnerable patient populations.
Multivariable analyses identified several predictors of anxiety reduction, including participation in the intervention group, female sex, high preexisting anxiety, and more complex anesthetic procedures. Notably, demographic and clinical factors such as age, ASA classification, and surgical type did not significantly influence whether anxiety increased following consultation, reinforcing the central role of communication in modulating patient experience.
What we think is remarkable about this study is that prior strategies to reduce anxiety include patient education, pharmacologic premedication, and psychological interventions. In contrast, this study demonstrates that a brief, 1-hour training session, a low-resource intervention targeting clinician communication can produce measurable improvements in patient outcome. Additionally, previous studies evaluating interventions to improve informed consent have generally failed to reduce patient anxiety and, in some cases, have increased it.3-5 The present findings suggest that the manner in which risk information is conveyed—particularly through positive framing and expectation management—may be more influential than the quantity of information provided. This aligns with evidence that nocebo effects are driven by negative expectations and can be mitigated through targeted communication strategies.
Finally, Dutton provides what we think is a fantastic table of his recommended simple steps to reduce preoperative patient anxiety (table below).
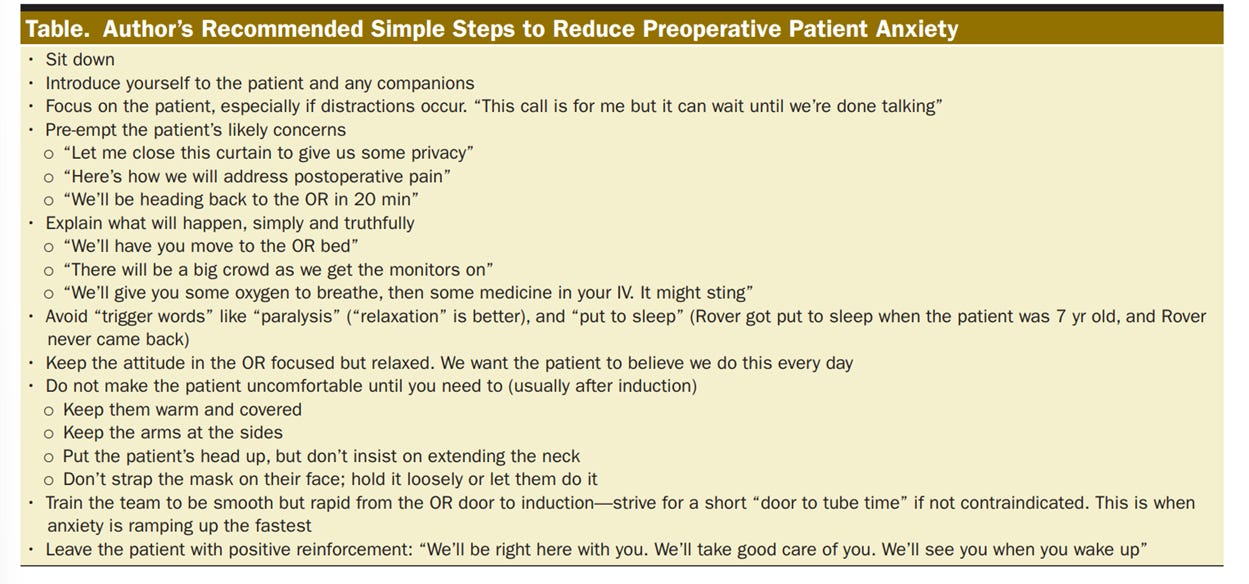
What to do if there is no chair available to ‘sit down’ on in the preoperative area? Perhaps attempt to be at eye level with the patient for even a short period of time, like bowing forward when introducing yourself, or squatting to a child’s level when addressing them.
Send your thoughts and comments to Myron (myasterster@gmail.com) and he will post in a Friday reader response.
References
1. Zech N, Bauer A, Hansen E. Communication Training for the Preoperative Anesthesia Consultation Reduces Anxiety: A Prospective, Patient-Blinded Pre-Post Intervention Study. Anesthesia and analgesia 2026;142(5):869–878. (In eng). DOI: 10.1213/ane.0000000000007791.
2. Dutton RP. Risk Without Terror in Anesthesia Consent. Anesthesia and analgesia 2026;142(5):866–868. (In eng). DOI: 10.1213/ane.0000000000007865.
3. Powell R, Scott NW, Manyande A, et al. Psychological preparation and postoperative outcomes for adults undergoing surgery under general anaesthesia. The Cochrane database of systematic reviews 2016;2016(5):Cd008646. (In eng). DOI: 10.1002/14651858.CD008646.pub2.
4. Kinnersley P, Phillips K, Savage K, et al. Interventions to promote informed consent for patients undergoing surgical and other invasive healthcare procedures. The Cochrane database of systematic reviews 2013;2013(7):Cd009445. (In eng). DOI: 10.1002/14651858.CD009445.pub2.
5. Kassahun WT, Mehdorn M, Wagner TC, Babel J, Danker H, Gockel I. The effect of preoperative patient-reported anxiety on morbidity and mortality outcomes in patients undergoing major general surgery. Sci Rep 2022;12(1):6312. (In eng). DOI: 10.1038/s41598-022-10302-z.