


Give me LIBERTY, or give me Death: ICU Liberation in Pediatric Critical Care
Kumaran Senthil, MD and Justin L. Lockman, MD MSEd

Original article
Fan E, Zakhary B, Amaral A, McCannon J, Girard TD, Morris PE, Truwit JD, Wilson KC, Thomson CC. Liberation from Mechanical Ventilation in Critically Ill Adults. An Official ATS/ACCP Clinical Practice Guideline. Ann Am Thorac Soc. 2017 Mar;14(3):441-443. PMID: 28029806.
The Society for Critical Care Medicine’s ICU Liberation campaign “aims to liberate [adult and pediatric] patients from the harmful effects of an intensive care unit stay” (https://www.sccm.org/ICULiberation).1 While many PAAD readers may not work in ICUs, it’s still important to be aware of this campaign because so many perioperative patients start and/or end in the ICU. Not to mention the role we anesthesiologists play in helping to meet all of the goals! The campaign includes a bundle of care elements including and not limited to: emphasizing assessment of pain with appropriate analgesia/sedation, spontaneous breathing trials to promote timely extubation, ICU delirium prevention and management, progressive mobility, and family engagement. Of the elements in the bundle, development of guidelines for pediatric ventilator liberation remains the most limited by inadequate data and considerable practice variation.
In 2017, the American Thoracic Society and American College of Chest Physicians collaborated to create clinical practice guidelines for liberation from mechanical ventilation in critically ill adults.2 Six year later, we are very excited that on behalf of the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network, clinical practice guidelines for pediatric ventilator liberation have now been published in the American Journal of Respiratory and Critical Care Medicine and endorsed by both the Society for Critical Care Medicine and the American Thoracic Society.3, 4
Due to the paucity of interventional trial data, these guidelines are based on expert consensus and low-quality evidence. Nonetheless, they emphasize fundamental principles that may not be evident across all pediatric intensive care units. Of note, these recommendations are intended for children (from 1 day to 18 years old) who have been intubated for at least 24 hours.
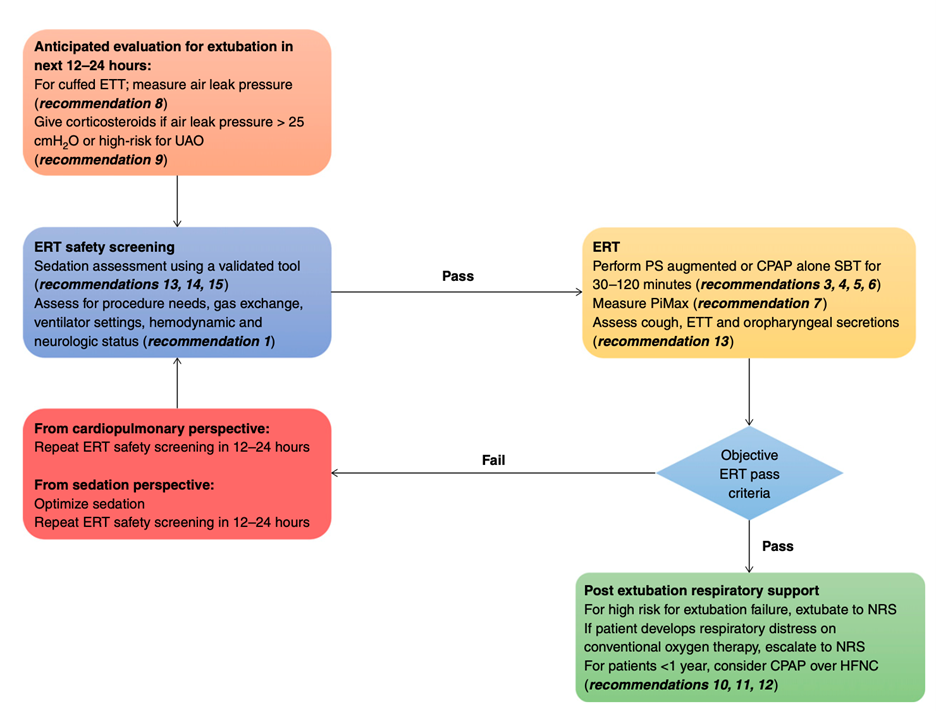
Most central is the recommendation for protocolization of both screening for eligibility for extubation readiness tests (ERTs) and of the extubation readiness test performance bundle itself, rather than just using “clinical assessment” to determine readiness. A spontaneous breathing trial (SBT) is suggested as a part of the ERT bundle, though SBT specifics are less well defined. For standard risk patients, guidelines suggest use of either CPAP with pressure support or pressure support only SBT, but for those at higher risk for extubation failure the recommendation is to use a more conservative CPAP only SBT.
An air leak test is recommended for all patients with cuffed endotracheal tubes, with dexamethasone administration at least 6 hours prior to extubation for those with a high leak pressure. Note that there were a few PAADs over the past few weeks talking about controversies surrounding the leak test. [See: https://ronlitman.substack.com/p/remembering-the-classics-the-leak and https://ronlitman.substack.com/p/the-leak-test-another-bubbameisa.] Post-extubation respiratory support should favor non-invasive respiratory support (high flow nasal cannula, CPAP or BiPAP) over conventional oxygen therapy, which may mask hypoventilation. Finally, although there is a suggestion for targeted sedation using a validated sedation tool, there are no data supporting a standardized sedation titration protocol despite two randomized controlled trials.5, 6 Sedation protocols may vary from those studied. An example of a Pediatric ICU Sedation Pathway developed at CHOP is available here: https://www.chop.edu/clinical-pathway/sedation-analgesia-picu-mechanically-ventilated-patient-clinical-pathway. The authors conclude these clinical practice guidelines with a flowchart that gives a helpful mental model for ventilator liberation in pediatric intensive care units:
These guidelines are an important synthesis of both expert consensus and existing, albeit modest, available data. Timely liberation from invasive mechanical support is necessary to facilitate discontinuation of sedatives with numerous side effects, promote physical rehabilitation and brain recovery, and decrease ongoing tracheal inflammation that may result in long term glottic and subglottic pathology. This must be balanced with premature extubation that may require re-intubation, or protracted courses of high levels of non-invasive respiratory support that may hinder rehabilitation in addition to risking both inadequate enteral nutrition and deforming skin injuries on the face.
This balance continues to be a point of contention nationally and internationally. If the threshold to extubate is too high, then extubation failure will become non-existent, but many will suffer the iatrogenesis of prolonged invasive mechanical support. If that same threshold becomes too low, then the pendulum swings in the other direction. An ideal target extubation failure rate (e.g., 15% of patient extubations should fail if we are extubating early enough) is undefined, or maybe it cannot be defined for our heterogenous population, in which case we should focus on subgroups. Such an optimal threshold would hopefully maximize ventilator free days, minimize ICU length of stay, and promote speedy recovery to baseline levels of respiratory and neurologic function.
The creation of these guidelines is a monumental first step in pediatric critical care to providing a framework for pediatric intensive care units, namely in protocolization of ERTs and supporting SBTs. The additional guidance is helpful and uncovers many opportunities of further study to add high quality data for future iterations in years to come. What do you think? Do you use ERTs and SBTs in your practice? Can SPA members collaborate to answer some of the above outstanding questions? Send your responses or other comments to Myron who will post them in a Friday Reader Response.
PS from Myron: A PICU special interest group led by Drs. Shawn Jackson, Tim Welch, and Branden Engorn has been reinvigorated at the Society for Pediatric Anesthesia. All SPA special interest groups are open to all members. If you are interested and/or in a combined Peds Anesthesia/PICU fellowship training program please contact Dr. Jackson (shwan.jackson@childrens.harvard.edu) and attend their meeting to be held at the SPA annual meeting in October.
References
1. Society for Critical Care Medicine. ICU liberation. Accessed 07/14/2023, https://www.sccm.org/iculiberation
2. Fan E, Zakhary B, Amaral A, et al. Liberation from Mechanical Ventilation in Critically Ill Adults. An Official ATS/ACCP Clinical Practice Guideline. Ann Am Thorac Soc. Mar 2017;14(3):441-443. doi:10.1513/AnnalsATS.201612-993CME
3. Abu-Sultaneh S, Iyer NP, Fernández A, et al. Operational Definitions Related to Pediatric Ventilator Liberation. Chest. May 2023;163(5):1130-1143. doi:10.1016/j.chest.2022.12.010
4. Abu-Sultaneh S, Iyer NP, Fernández A, et al. Executive Summary: International Clinical Practice Guidelines for Pediatric Ventilator Liberation, A Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network Document. Am J Respir Crit Care Med. Jan 1 2023;207(1):17-28. doi:10.1164/rccm.202204-0795SO
5. Curley MA, Wypij D, Watson RS, et al. Protocolized sedation vs usual care in pediatric patients mechanically ventilated for acute respiratory failure: a randomized clinical trial. Jama. Jan 27 2015;313(4):379-89. doi:10.1001/jama.2014.18399
6. Blackwood B, Tume LN, Morris KP, et al. Effect of a Sedation and Ventilator Liberation Protocol vs Usual Care on Duration of Invasive Mechanical Ventilation in Pediatric Intensive Care Units: A Randomized Clinical Trial. Jama. Aug 3 2021;326(5):401-410. doi:10.1001/jama.2021.10296