
Arterial catheter flushing practices – not so fast, kiddo!
Kelly Aluri MD and James Xie MD

Original article
Weber MD, Conlon TW, Zuckerberg JC, Himebauch AS, Senthil K. The Impact of Variable Arterial Catheter Flushing Practices on Flow Rates and Infusion Pressures. Anesth Analg. 2026 May 1;142(5):1028-1030. doi: 10.1213/ANE.0000000000007822. Epub 2025 Oct 24. PMID: 41980269.
You have just drawn an arterial blood gas and it’s time to flush the blood-filled line–do you pull the fast-flush tab or manually flush with a syringe? Are you thinking about your flush technique or what’s next on your task list? Flushing the arterial line is a part of the anesthesia workflow that can be overlooked and rushed for many reasons. Whether rushing to run a lab or feeling eager to see the blood pressure, anesthesiologists can easily default to a rapid manual flush.
We know that high flow rates through an arterial line can cause local injury, vasospasm, or embolism from retrograde arterial flow. Current literature suggests flow rates < 0.5 mL/sec can minimize risk of retrograde flow in neonates.1 However, there is little data and often little guidance during training on the optimal method of arterial line flushing. Closed blood sampling syringes (CBSS), such as Edwards Lifesciences’ VAMP system, pressure infuser bags, and syringe pump infusions are three commonly used arterial line set ups. There is limited research comparing the flushing mechanics of each system. Today’s PAAD2 explores the mechanical consequences of arterial line flushing and the clinical implications for how we flush arterial lines in the OR and ICU.
Weber et al.2 built a custom bench setup (Figure 1) to compare the flow rates and pressures of two flushing methods: CBSS versus pressure bags. They measured the flow rate using a micro-controller to precisely calculate the time required to flush 3 mL of fluid. They measured the pressure using a pressure sensor in series with the arterial catheter and used a mixture of glycerol and water to replicate the viscosity of blood. To evaluate CBSS systems which rely on variable human force, the authors built a hinged lever arm using weights to apply a measurable, consistent force to the CBSS. To evaluate the pressure bag fast-flush technique, they used bags of different fixed pressures.
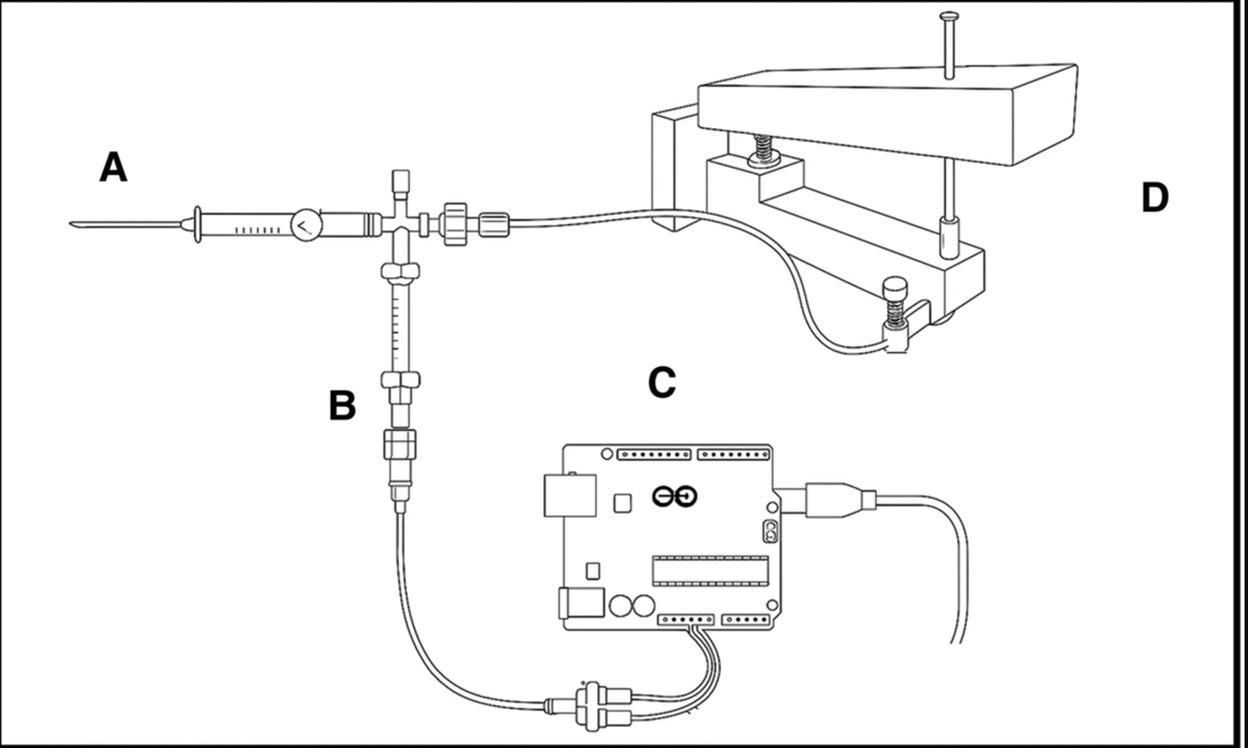
Figure 1 Schematic of mechanism to evaluate CBSS flushing dynamics. A, Arterial catheter. B, Harsh media pressure sensor. C, Arduino board. D, Hinged lever arm with mounted CBSS.
This in-vitro bench setup is quite clever, because replicating these high-pressure scenarios in real patients would be ethically and technically unfeasible.
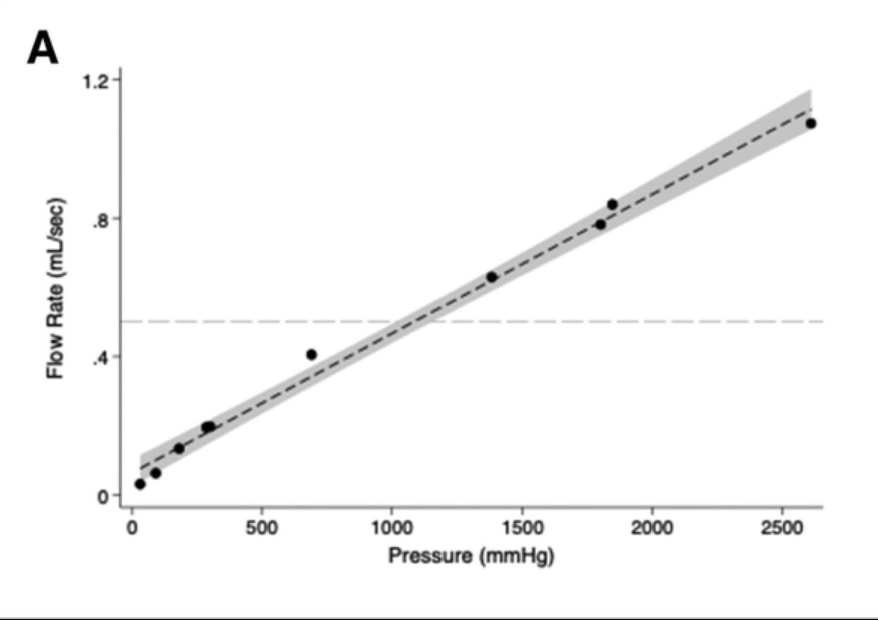
What did they find? With the CBSS system, the relationship between the flow rate and subsequent infusion pressure was linear (Figure 2A). Flow rates above 0.5 mL/sec generated a downstream pressure of > 1000 mmHg. This is a massive amount of pressure to introduce within a neonatal artery, where the baseline mean arterial pressure can be 30 to 50 mmHg. Furthermore, a previous study3 found that retrograde embolization of micro-air bubbles into the carotid artery occurred in 9 out of 16 patients when infusion pressure exceeded 1000 mmHg.
With the pressure bag system, flow rates depended on driving pressure (the difference between the infusion pressure and downstream pressure). All 3 set pressures (100, 200, and 300 mmHg), generated a flow rate < 0.3 mL/sec, which is within the current guidelines to minimize risk of retrograde flow.
Why does this matter? Manual syringe flushing may result in excessive flow rates and pressures that increase risk of retrograde embolic events. (See previous PAADs here and here), The risk may be even higher with axillary arterial catheters that are closer to the carotid artery.4 If a syringe-based flushing system is used, more diligent education for anesthesiologists and ICU nurses may be necessary to target flush rates <0.5 mL/s.
Does this mean pressure bags are always better? The authors state, “The use of a pressure bag removes the human factors that may contribute to excessive infusion pressures, and…may be a superior option to limit harm.” However, in the study they cited regarding retrograde flow, pressure bags set at 200 mmHg and 300 mmHg still caused retrograde flow in the subclavian artery 100% of the time. Even at the lower 200 mmHg setting, retrograde flow reached the carotid artery in one-third of cases (2 out of 6). If we can achieve a gentler and slower manual flush than the fast-flush tab, that may be optimal for preventing injury, but the impact of human error may render that unrealistic. It is important to keep in mind that different vendors of arterial line transducer flush tabs may have differently calibrated flow rates. For the most part, the nominal flow rate of a pressure bag setup is 3 mL/hr to keep the arterial line from clotting. Depending on which brand of flush tab you have, the rate can be anywhere from 30-60 mL/min to >120 mL/min (read your specific brand’s manual for use!)
Don’t forget infusion pump flush setups too!
A third arterial line set up (using an infusion pump), was not investigated in this study, but could provide an alternative solution. The benefit of this setup is that even lower rates of infusion than 3 mL/hr from the pressure bag can be dialed in, which is particularly helpful in neonates who have strict total fluid goals. Once a safe flush rate from a pump is established, a syringe pump can deliver a consistent rate, freeing up the clinician’s hands and cognitive load. Some centers where I (JX) trained specifically use syringe pump setups for arterial lines for this reason. In some cases, when infusions via the arterial catheter are greater than a nominal amount, the measured pressure may be affected. Thus, we recently did an in-vivo study to see whether the arterial line infusion rate affected the measured pressure, which it seemed it did - further emphasizing the point that we should really strive to understand how arterial line setups have clinical consequences!
Where does the research go from here? This study was solely in vitro, and previous in vivo studies on the consequences of arterial flushing are very small. Larger in vivo studies are likely necessary to establish more confident guidelines. There is also little research on how manual flushing and fast-flush techniques impact arterial vasospasm, arterial catheter-associated injuries, and arterial catheter longevity, which are other clinically relevant outcomes.
What can you do today? It’s important for anesthesiologists to understand CBSS (VAMP) systems, which are increasingly used in ICUs to reduce blood waste and the risk of catheter-associated infections. It’s also important for trainees coming to pediatrics after months of adult training to exercise caution when flushing arterial lines in babies (regardless of method). If there is an opportunity to change the default arterial line set up in your clinical setting, consider the pros and cons of each system. By understanding the implications of the flush setups we use (passive and active flush rates), we can be more mindful providers and minimize harm to patients.
Send your thoughts and comments to Myron (myasterster@gmail.com ) and he will post in a Friday reader response.
PS from Myron: I vividly recall the first percutaneous inserted intra-arterial catheter placements in pediatrics. I was a visiting medical student at the Children’s Hospital of Philadelphia (1975) and was spell bound as I saw one inserted in the radial artery by the attending, Dr. Russ Raphaely. Because so little was known about the safety and longevity of these catheters once placed, only attendings or fellows were allowed to sample arterial blood! Further, they used only glass, heparinized syringes and didn’t pull back on the syringe to withdraw blood. Rather, they insisted on using the native arterial blood pressure to fill the syringe! How times have changed!
References
1. Murphy GS, Szokol JW, Marymont JH, Avram MJ, Vender JS, Kubasiak J. Retrograde blood flow in the brachial and axillary arteries during routine radial arterial catheter flushing. Anesthesiology 2006;105(3):492–7. (In eng). DOI: 10.1097/00000542-200609000-00012.
2. Weber MD, Conlon TW, Zuckerberg JC, Himebauch AS, Senthil K. The Impact of Variable Arterial Catheter Flushing Practices on Flow Rates and Infusion Pressures. Anesthesia and analgesia 2026;142(5):1028–1030. (In eng). DOI: 10.1213/ane.0000000000007822.
3. Weiss M, Balmer C, Cornelius A, Frey B, Bauersfeld U, Baenziger O. Arterial fast bolus flush systems used routinely in neonates and infants cause retrograde embolization of flush solution into the central arterial and cerebral circulation. Canadian journal of anaesthesia = Journal canadien d’anesthesie 2003;50(4):386–91. (In eng fre). DOI: 10.1007/bf03021037.
4. Zaleski KL, Kuntz MT, Staffa SJ, Van Pelt H, Hamilton ARL, Atkinson DB. Central Arterial Line Placement for Pediatric Cardiac Surgery: A Single-Center Experience. Anesthesia and analgesia 2024 (In eng). DOI: 10.1213/ane.0000000000006972.