


Central arterial catheter placement in children: When it may be worth the risk
Myron Yaster MD, Ethan Sanford MD, Shawn Jackson MD PhD, Justin L. Lockman MD MSEd, and Genie Heitmiller MD

Occasionally, even with the use of ultrasound, peripheral arterial cannulation (usually the radial or ulna) is unsuccessful and consideration of central arterial access must be considered. Zaleski et al1 investigated the complications associated with central (axillary and femoral) arterial line placement in pediatric patients undergoing cardiac surgery.
To be honest, I (MY) was horrified when I saw this article and its advocacy of axillary line placement as I remember abandoning temporal arterial line placement in newborns because of the high risk of stroke development (figure below).2

Would the close proximity of the axillary artery to the aortic arch produce similar catastrophes? Indeed, because of this risk, I was always extremely careful in how I, or any of my students, flushed ANY arterial catheter, even radial artery catheters due to the risk of cerebral embolization.3 Has the time come for axillary arterial line catheters to become more common in the main pediatric ORs and the PICU? Myron Yaster MD
Original article
Zaleski KL, Kuntz MT, Staffa SJ, Van Pelt H, Hamilton ARL, Atkinson DB. Central Arterial Line Placement for Pediatric Cardiac Surgery: A Single-Center Experience. Anesth Analg. 2024 Jun 27. doi: 10.1213/ANE.0000000000006972. Epub ahead of print. PMID: 38935540.
In this single center (Boston Children’s Hospital), retrospective study, Zaleski et al. looked at complications (pulse loss, vascular compromise, or catheter-associated infection) in pediatric patients who underwent intraoperative placement of an axillary or femoral arterial line for cardiac surgery. “A total of 1263 central arterial lines were analyzed—195 axillary arterial lines and 1068 femoral arterial lines. The overall incidences of vascular compromise and pulse loss from central arterial-line placement were 17.8% and 8.3%, respectively. Axillary lines had lower rates of vascular compromise (6.2% vs 19.9%, P < .001), pulse loss (2.1% vs 9.5%, P < .001), and ultrasound-confirmed thrombus of flow abnormalities (14.3% vs 81.1%, P = .001) than femoral lines. Complications were more common in neonates and infants. By multivariate logistic regression, femoral location (odds ratio [OR], 4.16, 95% confidence interval [CI], 1.97–8.78), presence of a genetic syndrome (OR, 1.68, 95% CI, 1.21–2.34), prematurity (OR, 1.48, 95% CI, 1.02–2.15), and anesthesia time (OR, 1.17 per hour, 95% CI, 1.07–1.27 per hour) were identified as independent risk factors for vascular compromise. Femoral location (OR, 7.43, 95% CI, 2.08–26.6), presence of a genetic syndrome (OR, 1.86, 95% CI, 1.18–2.93), prematurity (OR, 1.65, 95% CI, 1.02–2.67), and 22-G catheter size (OR, 3.26, 95% CI, 1.16–9.15) were identified as independent risk factors for pulse loss.”1
The authors concluded that “axillary arterial access is associated with a lower rate of complications in pediatric patients undergoing cardiac surgery as compared to femoral arterial access. Serious complications are rare and were limited to femoral arterial lines in this study.”1
Several previous studies have investigated the safety of axillary arterial lines and found them to be safe and effective with few complications.4-7 In the most recent review, Gleich et al.4 found “the overall major complication rate of arterial cannulation for monitoring purposes in children is low (0.2%). All complications occurred in femoral arterial lines in children younger than 5 yr of age, with the greatest complication rates in infants and neonates. There were no complications in distal arterial cannulation sites, including more than 3,000 radial cannulations.”4 The Gleich study reported no complications in their subset of brachial/axillary arterial lines, but that cohort of 50 did not distinguish between axillary and brachial placement.
Based on today’s PAAD as well as prior publications, there is no evidence that the axillary artery is more dangerous than the femoral artery when it comes to central arterial cannulation. In fact, it may be safer as all four serious complications reported in the PAAD were from femoral catheters. However, it is important to remember that there were over five times the number of femoral catheters (n=1068) than axillary catheters (n=195) in the study. Therefore, it’s possible that the complication rate is similar, lower, or higher in axillary lines, and further study is needed to definitely answer this question. We do know that infants, in particular, tolerate loss of blood flow through the subclavian circulation. For example, the risk of serious complication to the arm with subclavian flap repair of aortic coarctation in infants is reported to be very low. So, hopefully, serious complications will remain at zero with the increasing use of axillary catheters. In the meantime, we see no reason from the existing evidence to avoid axillary arterial line placement in children when more distal sites are not able to be used.
In the ICU, we anecdotally note that axillary artery cannulation has become more common as a result of increasing comfort with the technique and the ubiquitous availability of ultrasound. While close monitoring to avoid potential complications remains important for all arterial lines, our (SJ and JLL) personal experience has been reassuring. All that being said, as the patient recovers, perfusion improves, and a peripheral arterial site becomes available, transitioning to a site with less risk seems prudent. In the meantime, we also remind readers that axillary is not brachial – the limited collateral flow around the brachial arterial likely makes that a much higher risk site and it should be avoided except in the most extreme situations.
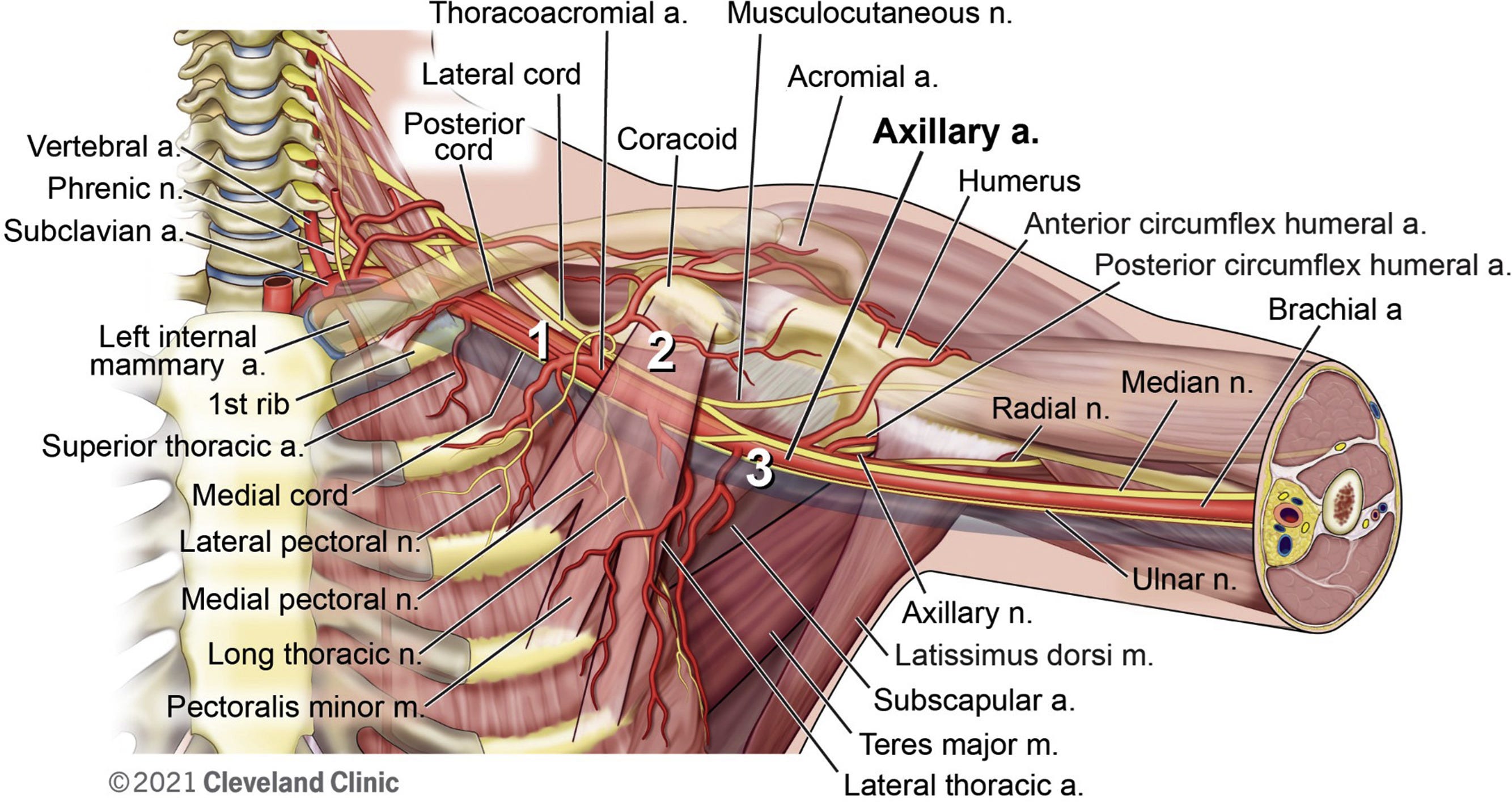
Seto et al. provide an excellent resource on best practices on how to perform percutaneous axillary artery access. They recommend using the 2nd segment of the axillary artery to avoid neurovascular complications (figure below).7 If you wish to take a deeper dive we highly recommend this article which also includes excellent ultrasound images to help guide you.
What do you do? Send your thoughts and comments to Myron at MYasterster@gmail.com who will post in a Friday Reader Response.
PS from Myron
In the PAAD, I raised many questions about the possible risks of retrograde cerebral embolization for a catheter so close to the aortic arch and in how these catheters are flushed. I asked several members of the PAAD’s executive council to weigh in and offer recommendations on how best to flush an arterial line catheter. Much to my surprise/shock/dismay/chagrin there was no consensus on a process that takes place daily in the ORs and ICUs. Because the P AAD has a worldwide audience and many practices like this are local, I’m asking you to submit how you do it and I will post in a Friday reader response.
PSS from Myron Hot off the presses: In another article of a critically ill pediatric cohort just published in the May issue of Pediatric Anesthesia, axillary arterial catheters were used longer and in a more severely ill population than radial catheters. Despite these differences, both catheter types demonstrated comparable safety and sustainability profiles.
Davidovich R, Kaplan E, Kadmon G, Nahum E, Weissbach A. Safety and Sustainability of Axillary Versus Radial Arterial Catheters in Critically Ill Children: A Retrospective Comparative Study. Paediatr Anaesth. 2025 May;35(5):389-393. doi: 10.1111/pan.15087. Epub 2025 Feb 20. PMID: 39976336.
References
1. Zaleski KL, Kuntz MT, Staffa SJ, Van Pelt H, Hamilton ARL, Atkinson DB. Central Arterial Line Placement for Pediatric Cardiac Surgery: A Single-Center Experience. Anesthesia and analgesia 2024 (In eng). DOI: 10.1213/ane.0000000000006972.
2. Simmons MA, Levine RL, Lubchenco LO, Guggenheim MA. Warning: serious sequelae of temporal artery catheterization. The Journal of pediatrics 1978;92(2):284. (In eng). DOI: 10.1016/s0022-3476(78)80027-4.
3. Lowenstein E, Little JW, 3rd, Lo HH. Prevention of cerebral embolization from flushing radial-artery cannulas. The New England journal of medicine 1971;285(25):1414-5. (In eng). DOI: 10.1056/nejm197112162852506.
4. Gleich SJ, Wong AV, Handlogten KS, Thum DE, Nemergut ME. Major Short-term Complications of Arterial Cannulation for Monitoring in Children. Anesthesiology 2021;134(1):26-34. (In eng). DOI: 10.1097/aln.0000000000003594.
5. Lawless S, Orr R. Axillary arterial monitoring of pediatric patients. Pediatrics 1989;84(2):273-5. (In eng).
6. Piotrowski A, Kawczynski P. Cannulation of the axillary artery in critically ill newborn infants. European journal of pediatrics 1995;154(1):57-9. (In eng). DOI: 10.1007/bf01972974.
7. Seto AH, Estep JD, Tayal R, et al. SCAI Position Statement on Best Practices for Percutaneous Axillary Arterial Access and Training. J Soc Cardiovasc Angiogr Interv 2022;1(3):100041. (In eng). DOI: 10.1016/j.jscai.2022.100041.