
Reader response
Myron Yaster MD

From James Xie, MD, Stanford University School of Medicine
Thank you for addressing this important issue on shared decision making about do-not-attempt-resuscitation (DNAR) orders in the perioperative period. I wanted to bring up a related issue that I know is a workflow issue across many healthcare systems. Specifically: 1) How are DNAR orders made apparent to all members of the healthcare team? 2) If DNAR orders are temporarily suspended in the perioperative period, how do all members of the healthcare team know that? 3) What defines the end of the perioperative period if DNAR orders are going to be resumed after the patient has completed their procedure?
Re question 1: unlike most adult hospitals, pediatricians might not be routinely asking about code status of a patient on admission so everyone defaults to full code unless a POLST (Physician Orders for Life Sustaining Treatment) has been filled out and the care team is informed of a patient/family's choice for their child to have treatment goals that may not involve resuscitation (DNR) or intubation (DNI). If treatment restrictions are in place, the primary team will place an order in the electronic health record and this is made apparent in the patient's electronic chart.
Re question 2: let's say the patient is being offered a surgical treatment requiring anesthesia that may benefit them or palliate symptoms. As the PAAD aptly describes, a shared decision with the patient/family should be arrived upon as to whether DNAR orders are temporarily suspended in the perioperative period (a reason to do so may be that easily reversible causes of respiratory failure or cardiac arrest could/should be treated and are in line with the patient/family's wishes). But here's the tricky part: who is responsible for changing the code status order in the EHR? The surgeon? The primary team? The anesthesiologist who had the conversation? If it is not changed, the EHR will still display the patient has DNAR orders in place. What if someone gives the anesthesiologist caring for the patient a break and the suspension of the DNAR wasn't mentioned.. and the patient goes into cardiac arrest while the original anesthesiologist is out of the room? The EHR will misleadingly state the patient is still DNAR, which my lead to a delay in resuscitation!
Re question 3: let's say the hospital did have a good workflow for displaying that the patient's DNAR orders are temporarily suspended and all resuscitative measures should be taken in the perioperative period. Hang on! What even is the perioperative period? Is it from premedication to the end of PACU stay? Perhaps beyond that if there's a reversible surgical complication within the first 24 hours? What if the post-op destination is the ICU and there isn't a well-defined "end of PACU" time? Who gets to decide this (obviously the patient/family should be involved) and how is it clarified (will the code orders be tied to specific phases of care, for example)?
This ended up being more questions than answers, but I do think it's important to tackle these related issues so that we can properly respect DNAR orders that patients/families may wish to have in place both before, during, and after anesthesia care. This is also a plug for why clinical informatics is so crucial in perioperative care!
From Ethan L Sanford, MD
Thanks for the time and consideration in writing this, James! I'll admit to being somewhat technology adverse when as relates to this topic. In Texas we are mandated to actually have a paper form signed by parents regarding limitations in care. This adds another layer to the complex reporting systems you have outlined regarding EMR.
In my opinion, some of the answers to your questions are possibly unpopular but are what the reality of these scenarios require. In reverse order:
Question 3: I think the time period for changes in DNAR orders should be defined by the anesthesiologist, treating team and the family/patient. The large majority of the time it should be when the anesthesiologists signs out care to the ICU or floor team. For instance, if I'm sedating for a chest tube I might recommend allowing intubation in the perianesthetic period only under emergent/reversible circumstance. But that would also necessitate a discussion that if intubated, the time-course for extubating may be prolonged or possibly never safely accomplished. If the chest tube is placed, no further anesthetic medications will be administered, and the patient has resumed baseline health and I've signed out the patient to the ICU then the pre-anesthetic wishes should be resumed asap which is what I would advise the parents. If the child decompensated afterward, then presuming the family is informed and agrees, the preop DNAR orders should be followed. If for the same chest tube the child was intubated during the anesthetic, I would talk with the PICU team and family afterward to outline recommendations going forward. Even more uncomfortable, if the family does not want their child intubated and they decompensate during the anesthetic, I think we must have some mechanism to communicate the scenario to the family, allow their presence if possible, and ensure all team members (this should occur with timeout) are in agreement that not intervening is appropriate. There are so many possible scenarios which might demand dynamic alteration and differences in planning. I wouldn't want to put people and families in the position of doing things because of arbitrary rules. I think this is sometimes frustrating as there is value in concrete do's and don'ts but I just think these scenarios are nuanced and, therefor, require nuanced approaches not amenable to set rules.
Question 2: I think execution of the agreed plan is an obligation of the person who made the plan. I do agree there is an opportunity to create EMR identifiers which are intuitive and simple which may help. However, in a goal-directed construct of decision making every possible intervention and situational permutation are not necessarily discussed. Therefore, creating a check list of all possible scenarios and interventions is impossible. In this reality, I think it's the obligation of the anesthesia to team to execute the plan regardless of breaks or the place on the revered out list.
Question 1: This should be my question to you. Agree especially for transitioning back from periop care to PICU/floor having some simply way to view what the orders were, how they were adapted, and when any changes elapse may be helpful. Obviously, a lot of this should be well described in the pre and post op anesthesia notes, but I recognize these may not always be remembered or looked at. The backend transition back to prior DNAR orders is especially critical
From Richard Mahon, D.O., Director of Quality and Safety, Department of Anesthesiology and Pain Medicine, Akron Children's Hospital, Adjunct Clinical Assistant Professor Anesthesiology, Ohio University Heritage College of Osteopathic Medicine
First, I would like to say thank you for choosing our recent publication in Pediatric Anesthesia to highlight and review. Although we are aware that preop/periop acetaminophen is not a novel concept, we were happy with our results and hope that it inspires other institutions to change their practice as well. I would, however, like to respond to a couple questions that you had about our QI project and add some clarity.
The biggest obstacle in the project was access to acetaminophen and the culture change of ordering and giving oral acetaminophen in preop. We did utilize postoperative acetaminophen in our PACU on occasion (about 4% of patients), but our preop areas are not a convenient walk to PACU (Post Anesthesia Care Unit) for acetaminophen, so we had to convince our Pharmacy to find space in the preop MedSelects and actually acquire a new preop MedSelect for our busy Outpatient Surgery Center.
We would have also liked to expand on our cost analysis, but institutional restrictions on publishing acquisition costs, and limitations on the length of the manuscript required us to eliminate some key dialogue and explanations. I can tell you that we have continued to see good results and slow steady improvement since the beginning of 2019.
To give an idea on Cost Analysis calculations - Based on the P charts and Monthly Patient Average Totals:
Pre-implentation Baseline (January-July 2019) = 640 monthly doses of acetaminophen in anesthesia (90% IV & 10% oral) = cost for IV @ Acetaminophen 100mg / 10mL syringe - $20.22 / syr = estimate average dosing of 483 mg = 20.22*4.83 = average cost of $97.6626/patient; Current oral doses @ average dose of 530.53 mg @ average cost of (liquid @ $2.82/patient (Acetaminophen 160mg / 5mL cup - $0.85 / 5mL cup and 3.31 5 ml doses to get to 530 mg) and tab = $0.06/patient d/t 2 tabs per patient
Unfortunately, we did NOT have access to the Adaptx software during our project but have limited access now due to our involvement with Project Spruce. Since 2019 till present, we have seen a total of just over 92,000 surgical patients, and happy to say that of the Acetaminophen we do give now post QI project, close to 78% are still getting the much less expensive Oral formulation, with a decrease in rescue IV opioid rates.
From Myron Yaster MD For more detailed information on how to do this, please contact Dr. Mahon RMahon2@akronchildrens.org
Many readers have asked me to provide some background information on the PAAD and who reads it. The timing is perfect. In this month’s issue of the journal Pediatric Anesthesia, Drs. Melissa Brooks Peterson, Justin Lockman, and I wrote a brief history of the PAAD and outlined some exciting new developments in our growth. Here goes:
“It is simply impossible for busy clinicians to keep up with relevant medical literature. Even a narrow-focused specialty like pediatric anesthesiology overwhelms our ability to “keep up” with novel medical breakthroughs, revisited research in the field, important quality improvement initiatives, interesting editorials, and updated clinical guidelines.”1 The late Dr. Ron Litman recognized this conundrum during the isolation of his own cancer treatment and set out to do something about it. He subsequently started the Pediatric Anesthesia Article of the Day (PAAD). His initial goal was to help provide concise summaries of important new articles for his colleagues at the Children's Hospital of Philadelphia (CHOP), while appropriately referencing works for readers who wanted to see the originals in their full form. After his death, some of his friends continued the PAAD in his honor as a free resource to the worldwide pediatric anesthesia community.
Ron chose to publish the PAAD in Substack. Built within the Substack app are analytic tools. I thought you might all be interested in seeing graphs of our growth and where are readers are located.
1. Brooks Peterson M, Yaster M, Lockman JL. The Pediatric Anesthesia Article of the Day (PAAD): A new solution to a ubiquitous problem. Paediatric anaesthesia 2024 (In eng). DOI: 10.1111/pan.14879.
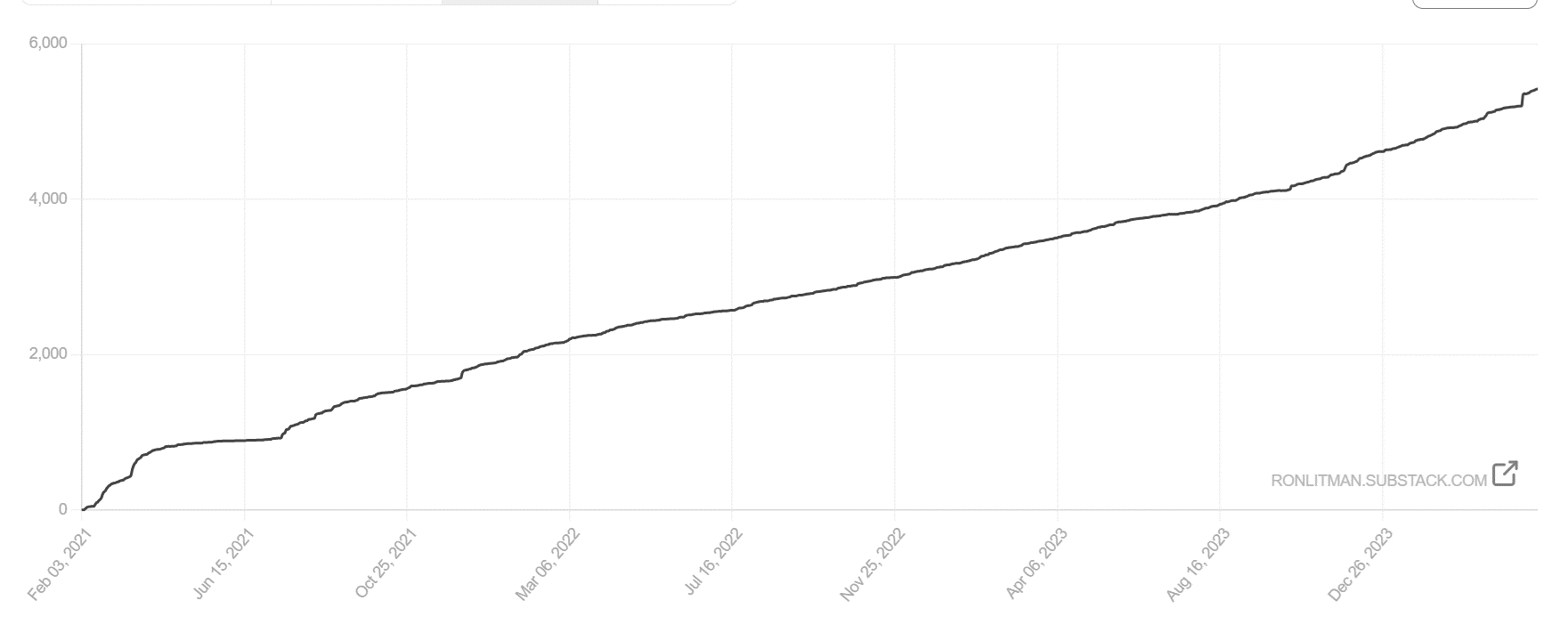
Total number of subscribers since the inception of the PAAD in 2020. At the time of his death, there were approximately 450 daily readers.
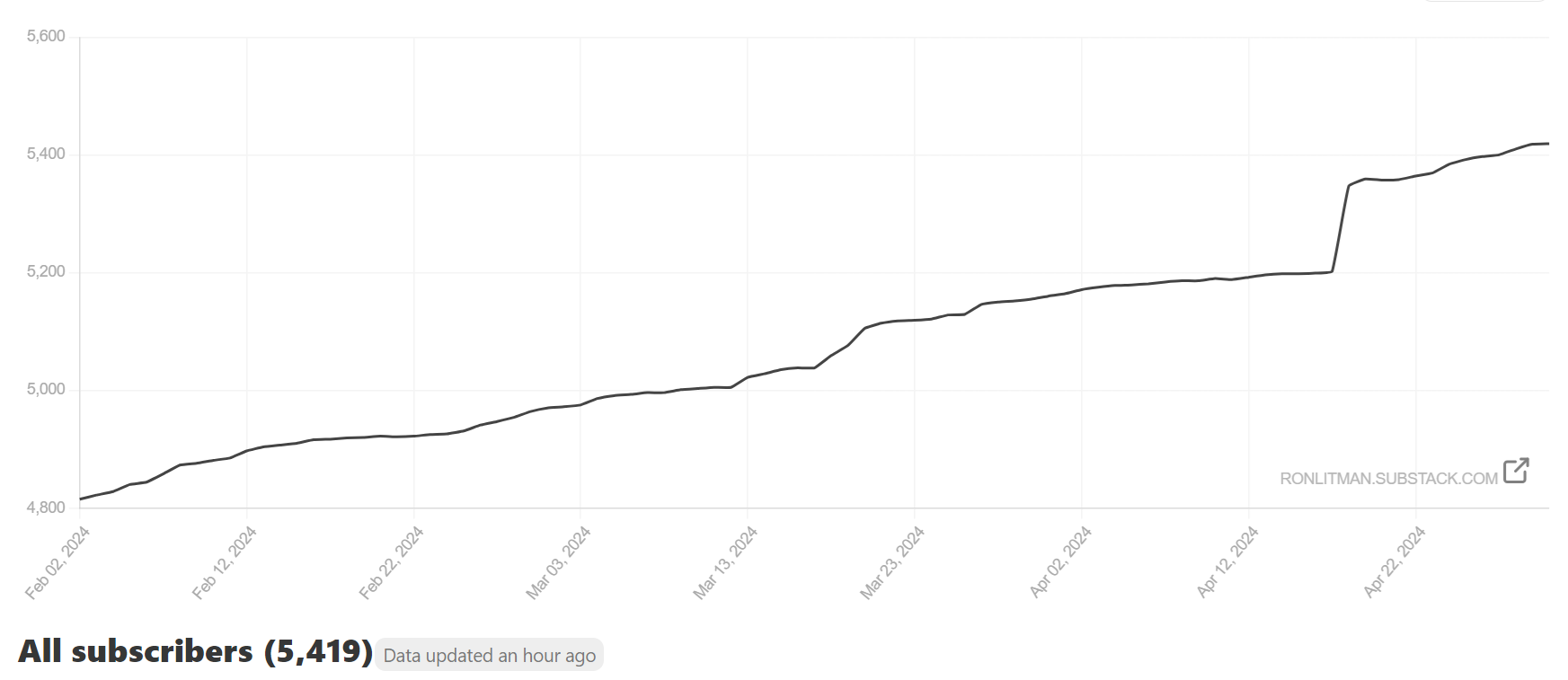
This graph represents the growth of the PAAD readership over the past 90 days. The large bump in April represents new readers primarily from the American Society of Dentist Anesthesiologists.
