


What an anesthesiologist should know about pediatric arrhythmias
Myron Yaster MD, Sean Barnes MD, MBA and Jamie McElrath Schwartz MD

Almost all of our American readers have been held hostage by their departments and credentialling committees and have been required/forced to take the American Heart Association’s Pediatric Advanced Life Support (PALS) course on a yearly or biannual basis to maintain their hospital privileges. To be honest, as a hostage, I never developed Stockholm syndrome and never really understood why I, as a pediatric anesthesiologist and lapsed intensivist, was forced to take PALS. Admittedly, it did give me the opportunity to review cardiac arrhythmias and practice using defibrillators.
Ah, defibrillators! For whatever reason, I simply could (and can) never remember how to set up and use the hospital’s biphasic defibrillators and whatever I learned while taking my PALS course evaporated from my memory within months of the training course. On the other hand, I did learn how to use out of the hospital, automated external defibrillators (AED), and on several occasions have used AEDs on “civilians” in air planes, concerts, and sporting events with great success. (My family believes that I am a CPR magnet!)
Which brings me to today’s PAAD by Kuntz et al.1 Identifying and treating pediatric arrhythmias is essential for pediatric anesthesiologists and today’s PAAD is essential reading. Because by design PAADs are brief 5-6 minute reads, our review will only scratch the surface of this article and I would urge all of you to read in its entirety and/or feature it in a journal club. Further, I think the management of pediatric arrhythmias should be considered as an addition to the PediCrisis app. After reading the article by Kuntz etal., I’ve asked the leaders of the PediCrisis app committee to consider adding this event to the app.
Finally, many of you when faced with patients with a history of arrhythmias defer to your colleagues in pediatric cardiac anesthesia, cardiac ICU, and pediatric cardiac electrophysiologists. However, because most pediatric patients present for anesthesia without a baseline electrocardiogram, the first identification of an arrhythmia may occur under general anesthesia. Therefore a basic knowledge of how to identify and treat these patients is essential. We will take a deeper dive later this month. Myron Yaster MD
Educational Review
Kuntz MT, Eagle SS, Dalal A, Samouil MM, Staudt GE, Londergan BP. What an anesthesiologist should know about pediatric arrhythmias. Paediatr Anaesth. 2024 Dec;34(12):1187-1199. doi: 10.1111/pan.14980. Epub 2024 Aug 15. PMID: 39148245.
In today’s PAAD, Kuntz et al. reviewed three common supraventricular tachycardia (SVT) mechanisms including 1. atrioventricular nodal reentrant tachycardia (AVNRT), 2. Wolff-Parkinson-White (WPW) syndrome, and 3. junctional ectopic tachycardia (JET). Additionally, the authors discussed two groups of patients at high risk for ventricular arrhythmias in the perioperative period: those with congenital long QT syndrome (LQTS) and catecholaminergic polymorphic ventricular tachycardia (CPVT).
Figure 1 provides a useful organizational framework for tachycardia, differentiating by the length of the QRS complex and regularity of the rate

The article then explores SVT in more depth.
“The most common pediatric tachyarrhythmia (estimated between 1 in 250 and 1 in 1000),2 SVT is a broad category of narrow complex tachycardias (Figure 1) initiated or maintained above the ventricular myocardium or His-Purkinje system.3 There are two primary mechanisms in pediatrics: reentrant (>90% of cases) and automatic (e.g., atrial tachycardia and junctional tachycardia).”1
In pediatric patients, pathologic SVT may be difficult to distinguish from sinus tachycardia. Characteristics which help differentiate sinus tachycardia from SVT are summarized in Table below

“Vagal maneuvers, such as Valsalva, carotid massage, and ice to face are not reliable, with reports of their efficacy varying between 25% and 75%. Adenosine, 1 or 2 doses, is approximately 70% effective in converting SVT to normal sinus rhythm. The usual first dose is 0.1 mg/kg, doubled for the second dose (max doses of 6 mg and 12 mg, respectively). The first dose is less effective in infants, and some recommend 0.2 mg/kg as the first dose. Adenosine failure can often be attributed to poor administration technique; adenosine's short half-life (<10 s) necessitates the medication to be pushed, followed by adequate flush.”1 Adenosine, rather than vagal maneuvers, is the preferred treatment for SVT in the hospital setting. As the authors note, administration technique is critical. If you haven’t given it before/recently, we suggest a consultation before giving it. Unstable SVT (shock, poor perfusion, falling ETCO2) should be treated with synchronized cardioversion.
The article has more discussions of Wolff-Parkinson-White syndrome (WPW), Junctional Ectopic Tachycardia (JET), long QT syndrome (LQTS), and catecholaminergic polymorphic ventricular tachycardia (CPVT). The discussion of LQTS is particularly helpful as it is a common pathology and many perioperative medications prolong the QT length. For the two cardiac anesthesiologists authoring this PAAD, we routinely use online resources to double check medications prior to anesthetizing a patient with LQTS.
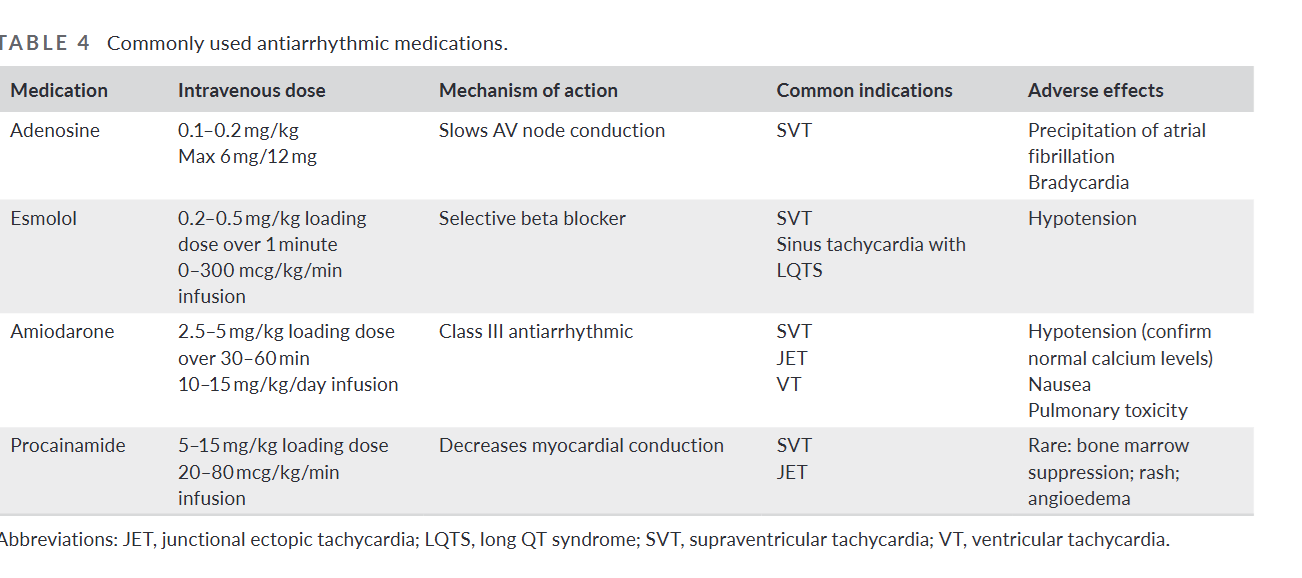
Anesthetics, surgical procedures, and vasoactive agents may precipitate perioperative arrhythmias. It is essential that you have understanding of the triggers, diagnosis and treatments of these arrythmias. Reproduced from the PAAD is this table on commonly used anti-arrhythmic medications.
Kuntz et al have provided us with a well-written review of arrhythmias that is useful for all anesthesiologists.
Do you feel comfortable treating these patients? Do you think this would be a good addition to the PediCrisis app? When you have an arrhythmia in the OR, do you manage alone or consult? Send your thoughts to Myron who will post in a Friday reader response.
References
1. Kuntz MT, Eagle SS, Dalal A, Samouil MM, Staudt GE, Londergan BP. What an anesthesiologist should know about pediatric arrhythmias. Paediatric anaesthesia 2024;34(12):1187-1199. (In eng). DOI: 10.1111/pan.14980.
2. Lewis J, Arora G, Tudorascu DL, Hickey RW, Saladino RA, Manole MD. Acute Management of Refractory and Unstable Pediatric Supraventricular Tachycardia. The Journal of pediatrics 2017;181:177-182.e2. (In eng). DOI: 10.1016/j.jpeds.2016.10.051.
3. Delacrétaz E. Clinical practice. Supraventricular tachycardia. The New England journal of medicine 2006;354(10):1039-51. (In eng). DOI: 10.1056/NEJMcp051145.