


Wednesday, March 17, 2021

In the March issue of A&A, Franz, et al. from Seattle Children’s have published their experience (i.e., QI initiative) trying to replace intraoperative and postoperative opioid administration with alternatives, such as dexmedetomidine, non-steroidal anti-inflammatories (NSAIDs), and/or regional analgesia, in their freestanding surgicenter. Their overarching goal was to determine whether it was possible to “minimize perioperative opioids in pediatric ambulatory surgical patients without compromising patient outcomes or value”. The team performed an 18-month-long QI improvement process, from January 2017 and June 2019, that included nearly 11,000 children for analysis. Their main intervention during that time was to replace intraoperative morphine and acetaminophen with dexmedetomidine and ibuprofen. This practice was based on their previous success reducing opioid use during tonsillectomy. The complete list of interventions are detailed in Table 1 of the publication.
By the end of the intervention phase, the group had impressively reduced intraoperative morphine use from 84% (297 ampules among 352 surgical cases) to 8% (32 opioid ampules among 393 cases) and postoperative morphine administration from 11% to 6%.
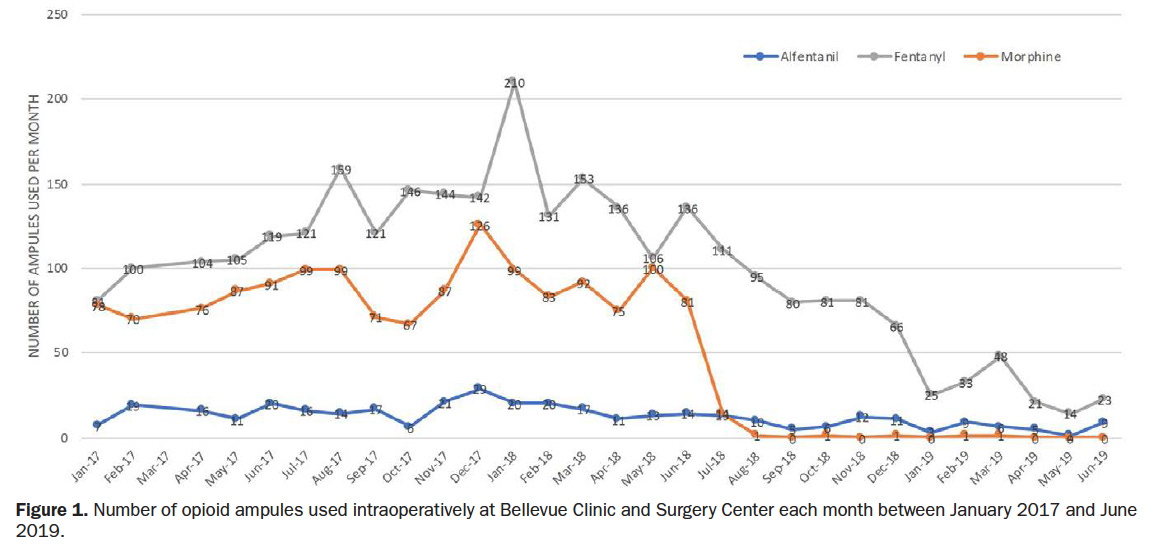
Figure from Franz, et al.
Although the paper is rife with run-time charts, it is very well written, and worth a careful look at those charts. The authors do a great job of explaining the many limitations of the data, which mainly center on changing circumstances and learning curves over time. Moreover, it is not possible from this study to determine important outcomes, such as the fate of these patients’ discomfort and opioid use after discharge. Or increased postoperative surgical bleeding from ibuprofen. Or patient and parent satisfaction, in the form of postoperative phone calls to the surgeon’s office.
Nevertheless, this is a train that has left the station on a national level, and we should all be evaluating similar metrics, and looking at the innovative practices at Seattle Children’s (and others I’m sure) to guide our own innovations. Congrats to the authors for presenting their data to our community. It’s the future of ambulatory pediatric anesthesia practice.
We should be careful not to swing the pendulum too far as is always done when something "new" comes up. There has not been any evidence that intraop opioids is an issue but rather postop. So though you need to plan for postop pain, avoiding opioids totally is not reasonable or feasible. I may be old school but I still give T&A patients opioids and so far there has not been any who had respiratory issues postop, even the ones who were admitted for overnight monitoring based on criteria (e.g., age, severe OSA, obesity). Caveat, everything should be administered judiciously and with thought.