


Tuesday March 16, 2021

Last month, while scanning the February issue of A&A for appropriate articles to review for PAAD, I came across a retrospective study authored by Wingert et al. about subtle findings of acute kidney injury (AKI) after non-cardiac surgery in children. They found that 3.2% of patients had laboratory evidence of AKI that did not exist preoperatively and discovered “significantly higher rates of mortality and 30-day readmission in multivariable, time-varying models with propensity-matched controls.” Although it was accompanied by a thoughtful editorial by Atkinson and DiNardo that described its limitations and potential for hypothesis-generating studies of the future, I brushed it off as too weak a study to include in PAAD. But as Issac Asimov once said, “the classic phrase of discovery in science isn’t “Eureka!” It’s more like “Hey, wait a minute….”
I thought of that quote, and the Wingert study, when I read the article by Su et al. in this past week’s issue of Jama-Open. The objective of Su’s study was to determine the association between ibuprofen prescriptions and the risk of hospital acquired AKI in hospitalized children in China. Ibuprofen inhibits prostaglandin synthesis, which leads to preglomerular vasoconstriction, and decreased renal perfusion.
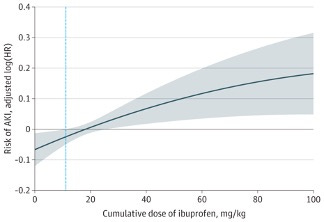
The authors examined a database of over 3 million patients admitted to 25 academic medical centers from 2013 to 2015. Among those patients, they found over 50,000 children who qualified for analysis. Of those, 5,526 (11.0%) used ibuprofen and 3,476 (6.9%) developed hospital-acquired AKI during hospitalization, as defined by an increase in serum creatinine level more than 50% over the baseline value. After adjusting for confounders, ibuprofen use was associated with a greater hazard in children who had chronic kidney disease, required ICU admission, and were greater than 10 years old. A dose-response analysis showed that the association of ibuprofen with the risk of hospital-acquired AKI was dose-dependent:
So, what can we learn from these two retrospective database studies, and how can they affect our practice of pediatric anesthesia? For now, not much. As Carl Sagan said, “Extraordinary claims require extraordinary evidence.” (Sorry, no more quotes for today) But, children taking ibuprofen preoperatively are not taking it for no reason – that very fact complicates any attempt to remove bias from a retrospective database study, no matter how large. There are countless reasons and comorbidities that accompany ibuprofen prescriptions that we can’t possibly account for.
What we can do, however, is think about the possible ramifications of preoperative ibuprofen use (Su et al.) and intraoperative hypotension (Wingert et al.) on susceptible anesthetized children, and how we can change their postoperative outcomes. We obviously can’t do a prospective study that randomizes children to ibuprofen or control prior to surgery, and then determine which group gets more AKI. It would be just as unethical to randomize children who were taking ibuprofen preoperatively to different blood pressure target ranges during surgery, and determine which group has the most AKI. But we can perform longitudinal observation studies that prospectively monitor kidney function before and after surgery to better define the problem and determine possible future interventions. We should figure out whether this problem really exists for the children we anesthetize. This is a good time for those kinds of studies, while equipoise still exists.
I think it’s important to keep in mind these studies and their findings. Make a mental note when a child has been taking ibuprofen preoperatively. And maybe follow creatinine levels postoperatively if risk factors are present.