
Time to Get on Board the Percutaneous Train; The Future is Going to Be Increasingly Non-Surgical
James DiNardo, Viviane Nasr, Lindsey Loveland Baptist, Susan Nicolson

Original article
Smith CL, Dori Y, O’Byrne ML, Glatz AC, Gillespie MJ, Rome JJ: Transcatheter Thoracic Duct Decompression for Multicompartment Lymphatic Failure After Fontan Palliation. Circ Cardiovasc Interv. 2022 Jul;15(7):e011733. doi: 10.1161/CIRCINTERVENTIONS.121.011733. Epub 2022 Jun 16. PMID: 35708032
The Fontan procedure was developed as a palliative intervention for CHD patients with single-ventricle anatomy who are not candidates for a biventricular repair. The surgery creates a series systemic and pulmonary circulation with the energy necessary to provide gradient-driven pulmonary blood flow generated by the ventricle. In the past decades, improvements in the surgery and medical management of these patients have increased survival, with 30-year survival rates close to 85%. Despite these improvements, this population remains at risk for complications and end-organ dysfunction due to Fontan failure, which is characterized by elevated systemic venous pressures and low cardiac output. These complications include arrhythmias, cardiac dysfunction, liver fibrosis/cirrhosis, renal dysfunction, pulmonary failure, and lymphatic complications such as edema, pleural effusions, ascites, plastic bronchitis (PB), and protein losing enteropathy (PLE).1
Lymphatic vessels participate in maintaining a fluid balance within the extracellular space by returning filtered proteins and fluid to the vasculature. The lymphatics also participate in fat reabsorption from the small intestine and play an important role in the body’s immune response. Eight-to-12 L of fluid and protein per day that otherwise would accumulate in extravascular compartments are returned to the bloodstream through the lymphatic system. Because systemic venous pressure is elevated in the Fontan circulation lymphatic drainage into the systemic venous circulation via the thoracic duct (normally located at the junction of the left internal jugular vein and innominate vein), is impaired by elevated lymphatic afterload.
While lymphatic embolization techniques have resulted in successful treatments for PB and PLE2 they have been less successful in treatment of multicompartment lymphatic failure defined by the presence of 2 or more of the following: PB, PLE, ascites, or pleural effusions. One innovative approach to this problem has been to reroute drainage of the thoracic duct from its location into the high pressure systemic venous circulation to the lower pressure common atrium by detaching the innominate vein from the central circulation and anastomosing it to the common atrium.3
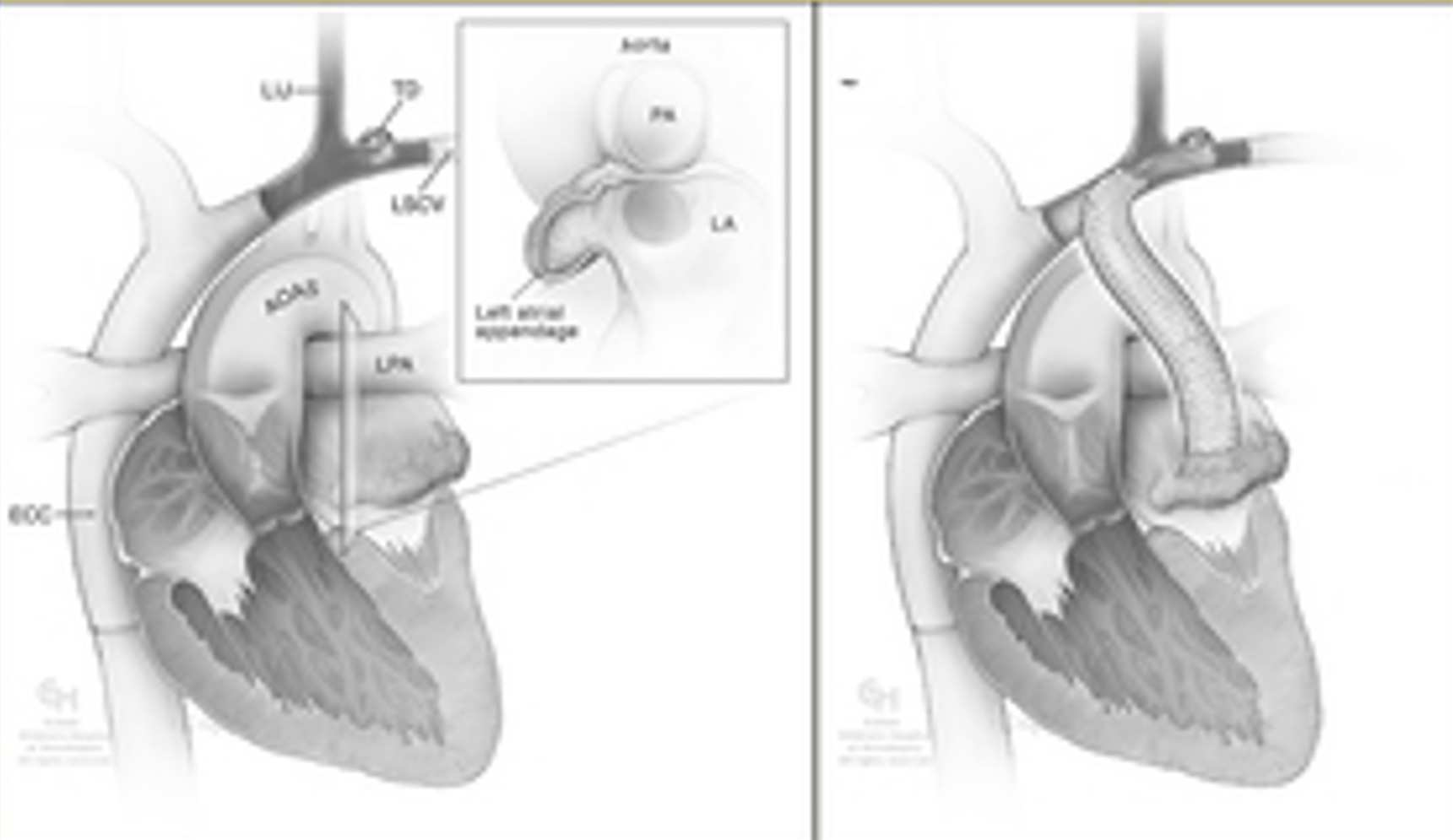
In the study presented in today’s PAAD, a non-surgical approach to this solution called transcatheter thoracic duct decompression (TDD), is described.4 Initially covered stents were used to channel the innominate vein flow inside of the cavopulmonary pathway into the pulmonary venous atrium. Subsequently a modified approach was developed where covered stents redirected innominate vein directly to the left atrium via an extravascular course (figure). TDD was performed by the innominate vein intra-Fontan tunnel technique in 4 patients, extravascular covered stent from innominate vein to atrium in 4, covered stent from left SVC to left atrium in 3, and perforation with stenting of an atretic coronary sinus in one.
Remarkably, there were no major procedural complications; 6 patients underwent subsequent procedures, most commonly to treat endoleaks. Lymphatic failure resolved in 6 patients, improved in 2, and was unchanged in 4 at 6 (range: 1–20) months follow-up. One patient died after TDD from Fontan failure.
This report is important for several reasons. It demonstrates that the technical ability and imagination of our interventional cardiology colleagues is such that we should expect continued advances to be made in the non-surgical treatment of complex cardiovascular problems. A pediatric cardiovascular anesthesia program that does not embrace support of catheter-based interventions and advanced imaging techniques will be left behind. There is no longer any place for an aversion to “working in the cath lab”. In fact, in many busy programs, 2/3 of the total clinical load is providing anesthesia care to patients in the cardiac catheterization and electrophysiology laboratories, and in advanced non-invasive imaging areas. The combination of these patient’s cardiac physiology, resultant morbidities and perturbations imposed by the transcatheter interventions not infrequently requires greater integration of change and rapid response than bypass cases.
We have an obligation to our pediatric cardiac anesthesia trainees to assure that they obtain adequate clinical exposure to these innovative procedures, many of which are high-risk, to be capable of providing expert care once their training is complete.
From Myron:
In a recent PAAD (May 4, 2022), Drs. Susan Nicolson and Lindsey Loveland-Baptist, who together with Drs. Jim DiNardo and Viviane Nasr make up the PAAD’s cardiac writing team wrote: “With advances in surgical and catheter-based interventions and imaging modalities in patients with congenital heart disease (CHD), the practice of pediatric cardiac anesthesiology has evolved in parallel with pediatric cardiac surgery and pediatric cardiology as a distinct subspecialty. Since the 1st pediatric cardiac surgical procedure performed in 1938, the training of pediatric cardiac anesthesiologists has evolved beyond that required of either a general, pediatric or an adult cardiac anesthesiologist. Through the early 2000s, anesthesiologists interested in practicing pediatric cardiac anesthesia gained additional training during their anesthesia residency, general pediatric anesthesia fellowship and/or as a staff member under the tutelage of an experienced colleague(s). Currently there is an ACGME accredited 2nd year advanced 12 months pediatric cardiac anesthesia fellowship with training milestones”.5
OK, here’s my question to you and I’ll post your responses in a future PAAD: Who should be doing these cath lab cases? Does it require a peds cardiac trained individual? In other words: should these cases be restricted to pediatric cardiac anesthesiologists (like bypass cases) or should ALL pediatric anesthesiologists be able to do them? Ditto for other imaging studies (MRI)? Ditto for non cardiac surgery, like an appendectomy? What physiology is the “line in the stand”?
References:
1. RochéRodríguez M, DiNardo JA. The Lymphatic System in the Fontan Patient-Pathophysiology, Imaging, and Interventions: What the Anesthesiologist Should Know. Journal of cardiothoracic and vascular anesthesia. Aug 2022;36(8 Pt A):2669-2678. doi:10.1053/j.jvca.2021.07.049
2. Dori Y, Keller MS, Rome JJ, et al. Percutaneous Lymphatic Embolization of Abnormal Pulmonary Lymphatic Flow as Treatment of Plastic Bronchitis in Patients With Congenital Heart Disease. Circulation. Mar 22 2016;133(12):1160-70. doi:10.1161/circulationaha.115.019710
3. Hraska V, Mitchell ME, Woods RK, Hoffman GM, Kindel SJ, Ginde S. Innominate Vein Turn-down Procedure for Failing Fontan Circulation. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2020;23:34-40. doi:10.1053/j.pcsu.2020.01.002
4. Smith CL, Dori Y, O'Byrne ML, Glatz AC, Gillespie MJ, Rome JJ. Transcatheter Thoracic Duct Decompression for Multicompartment Lymphatic Failure After Fontan Palliation. Circ Cardiovasc Interv. Jul 2022;15(7):e011733. doi:10.1161/circinterventions.121.011733
5. Nasr VG, Guzzetta NA, Miller-Hance WC, et al. Consensus Statement by the Congenital Cardiac Anesthesia Society: Milestones for the Pediatric Cardiac Anesthesia Fellowship. Anesthesia and analgesia. Jan 2018;126(1):198-207. doi:10.1213/ane.0000000000002482