


The impact of neurologic comorbidity on postoperative respiratory failure and mortality
Myron Yaster MD, Ethan L Sanford MD, Shawn Jackson MD PhD, Justin L Lockman MD MSEd

Original article
Mpody C, Kidwell RC, Willer BL, Nafiu OO, Tobias JD. Preoperative neurologic comorbidity and unanticipated early postoperative reintubation: a multicentre cohort study. Br J Anaesth. 2024 Nov;133(5):1085-1092. doi: 10.1016/j.bja.2024.08.006. Epub 2024 Sep 20. PMID: 39304468.
Children with neurologic comorbidities, especially those with cerebral palsy, seizure disorders, and/or neuromuscular disorders, are at increased risk of developing postoperative anesthetic and surgical complications – particularly pneumonia and respiratory failure requiring mechanical ventilation.1,2 Using the National Surgical Quality Improvement Program- Pediatric (NSQIP) database,3 Mpody et al. wondered (1) whether patients with preexisting neurological comorbidities would have more unanticipated early (< 72 hours) tracheal reintubations than the general pediatric population, and (2) would 30 day mortality be increased for this cohort?
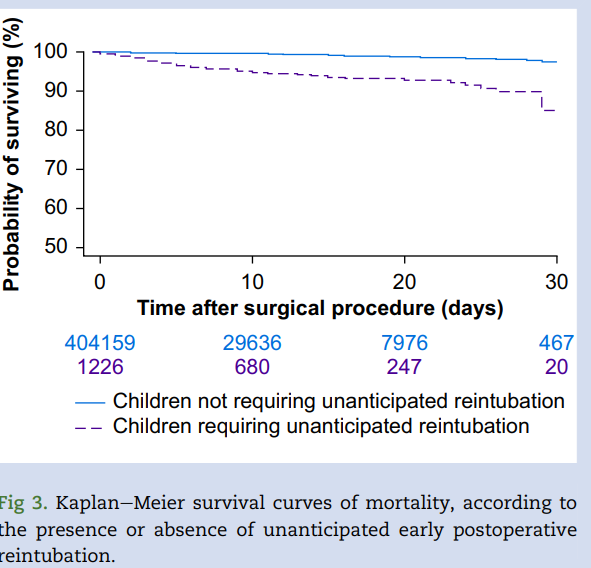
This multi-centered, retrospective study included 420,096 children who underwent inpatient, elective, noncardiac surgery at National Surgical Quality Improvement Program reporting hospitals between 2012-22. The patients with neurologic comorbidities were further subgrouped into: (1) structural central nervous system (CNS) abnormalities, (2) cerebral palsy, (3) seizure disorders, and (4) neuromuscular disorders. Their findings? “Cerebral palsy was associated with the highest risk of early reintubation (adjusted relative risk [RRadj]: 1.97, 95% confidence interval [CI]: 1.44-2.69; P<0.01), followed by seizure disorders (RRadj: 1.87, 95% CI: 1.50-2.34; P<0.01), neuromuscular disorders (RRadj: 1.76, 95% CI: 1.41-2.19; P<0.01), and structural central nervous system abnormalities (RRadj: 1.35, 95% CI: 1.13-1.61; P<0.01). Unanticipated early postoperative reintubation was associated with an eight-fold increase in 30-day mortality (adjusted hazard ratio: 8.1, 95% CI: 6.0-11.1; P<0.01). Risk of prolonged postoperative mechanical ventilation was also increased with neurologic comorbidities, particularly seizure disorders (RRadj: 1.73, 95% CI: 1.55-1.93; P<0.01).”2
Are any of you surprised by these findings? The increased risk of postoperative respiratory failure, need for reintubation and the risk of prolonged mechanical ventilation is well known in these cohorts and didn’t surprise us. In fact, many children’s hospitals work diligently to identify these patients for peri-operative optimization long before the day-of-surgery due to the increased risk. However, the dramatically increased risk of death within 30 days of surgery was a surprise – although maybe it shouldn’t have been since there is such a paucity of data on perioperative death beyond 7 days. This is particularly troubling for us as pediatric anesthesiologists as the anesthetic has become just as implicated (if not more so!) as the surgery itself.
There is certainly a need for future studies or management strategies to prevent harm for patients with these neurological comorbidities. Some strategies proposed by the authors include more comprehensive preoperative pulmonary care and nutritional support. 2 The intraoperative management also deserves consideration. For example, these children have different brain function and we have few to no data about disease-specific MAC, opioid requirements, etc. Basic pulmonary care such as careful endotracheal tube suctioning and recruitment maneuvers and forced coughing on extubation are likely critical in this population as well. Should we increase the use of regional anesthesia to minimize postoperative respiratory depression? The population of children with neurologic comorbidities is growing. These children require more anesthetic care and are at high risk for complications and death. The differences in function and physiology in these patients likely mandate special considerations for anesthetic care throughout the perioperative period. An important question that we can’t yet answer: Would the risk still be increased among these patients if their care were optimized (i.e., is the current care not optimized)? Or is the care optimized and they have increased risk nonetheless.
What do you think? How do you optimize the care for this patient population? What can SPA do to facilitate a multicenter study to answer these important questions? Send your thoughts and comments to Myron who will post in a Friday Reader Response.
References
1. Owusu-Bediako K, Mpody C, Iobst C, Tobias Joseph D, Nafiu OO. Risk assessment of postoperative pneumonia in children with neurologic disorders and obesity. Pediatric Anesthesia 2023;33(2):160-166. DOI: https://doi.org/10.1111/pan.14593.
2. Mpody C, Kidwell RC, Willer BL, Nafiu OO, Tobias JD. Preoperative neurologic comorbidity and unanticipated early postoperative reintubation: a multicentre cohort study. British journal of anaesthesia 2024;133(5):1085-1092. (In eng). DOI: 10.1016/j.bja.2024.08.006.
3. Raval MV, Dillon PW, Bruny JL, et al. Pediatric American College of Surgeons National Surgical Quality Improvement Program: feasibility of a novel, prospective assessment of surgical outcomes. Journal of Pediatric Surgery 2011;46(1):115-121. DOI: https://doi.org/10.1016/j.jpedsurg.2010.09.073.