


The anesthesia workforce: Supply demand imbalance part one
Myron Yaster MD, William J. Greeley MD, Aubrey Maze MD, and Joseph Carvero MD

“No matter what anyone says, it’s always about money” Mark Rogers MD
Just about every day, I get a despairing phone call from one of my friends about the anesthesia work force supply and demand imbalance, the death knoll of academic anesthesia practice, the “insane” and “unsustainable” salary demands of physician anesthesiologists and CRNAs, the loss of professionalism, acute and chronic staffing shortages in every type of practice, the increasing use of very expensive locum tenens coverage to fill staffing gaps, staff burnout, and a perceived death spiral of compromised healthcare access, quality, and safety. I’m sure you all are experiencing and talking about these issues as well.
Today’s PAAD by Abouleish et al.1 “focuses on the anesthesia workforce in the United States; it provides an overview of current workforce trends and challenges; and suggests potential solutions to meet the perioperative healthcare needs of our patients.” It does not deal with pediatric anesthesiologists per se2, nor the special workforce issues in pediatric cardiac anesthesia,3 nor problems in low and middle income countries.4 This is such an important topic that I assembled a group of leaders who have thought and dealt with these issues for a very long time in order to help me with the review of this paper. I’m hoping it will spur your thinking and be the basis of a future SPA roundtable. Indeed, I would urge all of you to read the article in its entirety and I am breaking it into 2 parts to allow a thorough review and still keep the PAAD to a 5-7 minute read. Myron Yaster MD
Original article
Abouleish AE, Pomerantz P, Peterson MD, Cannesson M, Akeju O, Miller TR, Rathmell JP, Cole DJ. Closing the Chasm: Understanding and Addressing the Anesthesia Workforce Supply and Demand Imbalance. Anesthesiology. 2024 Jun 17. doi: 10.1097/ALN.0000000000005052. Epub ahead of print. PMID: 38884582.
“The imbalance in anesthesia workforce supply and demand has been exacerbated post-COVID due to a surge in demand for anesthesia care, especially in non–operating room anesthetizing sites, at a faster rate than the increase in anesthesia clinicians. The consequences of this imbalance or labor shortage compromise healthcare facilities, adversely affect the cost of care, worsen anesthesia workforce burnout, disrupt procedural and surgical schedules, and threaten academic missions and the ability to educate future anesthesiologists. In developing possible solutions, one must examine emerging trends that are affecting the anesthesia workforce, new technologies that will transform anesthesia care and the workforce, and financial considerations, including governmental payment policies. Possible practice solutions to this imbalance will require both short- and long-term multifactorial approaches that include increasing training positions and retention policies, improving capacity through innovations, leveraging technology, and addressing financial constraints.”1
I (MY) have long taken the biblical view that the anesthesia workforce was akin to what Joseph told Pharaoh: “seven years of abundance would be followed by seven years of famine (Genesis 41:28–32).” In our professional lifetimes, we’ve lived through at least 2 of these workforce booms and busts. Perhaps the most profound and notorious bust occurred in the late 1990s following the 1995 article in the Wall Street Journal which predicted a glut of anesthesiologists and a shrinking marketplace.5 (In preparation for today’s PAAD, I (MY) reread the Anders’ article in the Wall Street Journal and I’d urge you all to read it too). What happened next was predictable and nothing short of a disaster. Medical students simply stopped applying and going into anesthesiology. Most anesthesia training programs did not fill and some residents in training switched from anesthesiology to emergency and family medicine! Within just a few years the resultant catastrophic shortage of staff anesthesiologists became profound. Academic and private practices did not have enough people to meet the demands of the operating rooms. Practices poached other practices for staff, signing bonuses became routine, academic physicians lost their non clinical time, academic practices became shells of their former selves. The famine and market forces then drove salaries to soaring new levels and surprise, surprise, medical students returned and anesthesiology became a desired profession once again. The same thing occurred just recently in pediatric anesthesia when Muffly et al. 2 predicted an oversupply of pediatric anesthesiologists, the seven years of plenty. Fellowship applications predictably fell dramatically6 and we are now entering the seven years of famine.
Covid 19 threw a monkey wrench into the system. “Before the pandemic, 35% of facilities reported an anesthesia staffing shortage. Two years after the pandemic, the percentage of facilities with a staffing shortage doubled to an astounding 78%.”7 This resulted in a dangerous spiral of work intensity and stress, unsustainable workloads, and retirements from clinical practice. The consequences of this “dangerous spiral” compromised healthcare access, quality, and safety and produced the healthcare crisis we are currently experiencing.”1
This problem is not unique to anesthesiology. Our good friend Dr. David Nichols, the former president of the American Board of Pediatrics told Myron in a personal communication that the same thing is happening in Pediatrics but worse. And we’ve all seen the shortages in nursing and other hospital staffing and how it is affecting medical practice and labor force economics. (WJG) Indeed, the results of this year’s residency match program is sobering and showed a more than 6% drop in medical student applications for Pediatrics where 30% of pediatric training programs failed to fill their available slots! As a direct result, there is a waning interest in pediatric subspecialties as well as the need grows. (We’ll have much more to say about Pediatrics in the next few weeks).
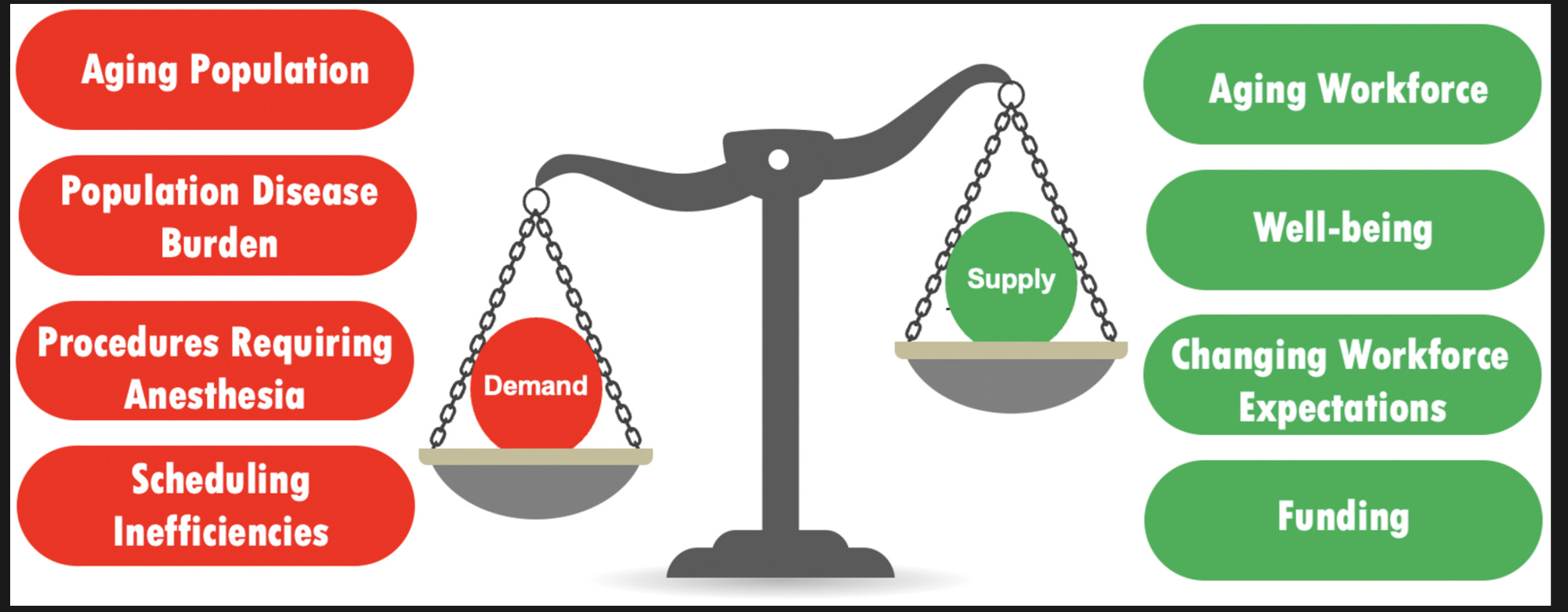
In anesthesia, the demand and supply side of the equation has/was changing even before COVID but COVID made it worse. In today’s PAAD we will focus on the supply side. In tomorrow’s we will concentrate on the demand side and possible solutions.
Supply side
“The Center for Anesthesia Workforce Studies estimates that 5,200 anesthesia professionals entered the workforce from training programs in 2023, comprising roughly 1,900 anesthesiologists, 3,000 nurse anesthetists, and 300 anesthesiologist assistants. At the same time almost 4,800 anesthesia professionals left the workforce in 2022, including 2,500 anesthesiologists 2,200 nurse anesthetists, and 65 anesthesiologist assistants. Although there is a net increase in workforce supply, demand for the number of procedures, increasing medical complexity, and inefficiencies in scheduling will continue to strain resources. ”1 (JC) As an Anesthesiology specialty we are facing a huge issue with a LACK of anesthesia resident trainees choosing to pursue fellowship training in pediatric anesthesia. We assume that this is because of the immediate, significant, financial pressures on this generation of trainees (loans and high cost of living) together with the incredibly rich contracts they are being offered as a general anesthesiologist. Perhaps the current generation is just not as interested in the sacrifices that need to be made to pursue an academic career? It would not be an overstatement to describe this as an existential threat to our profession. We (as leaders) need to do a better job of selling the value proposition of an academic fellowship in our specialty – the opportunities for creating new knowledge, the rewarding clinical practice, and the long-term financial benefits. In addition, we will need to look at alternative means of financing these fellowships in the short term. Do we identify talent and financially support those individuals (with faculty salaries) during a fellowship with a quid pro quo that the trainee with commit to working for our department as a subspecialist for some period of time in repayment of that support?
Why are so many leaving the profession? “The anesthesia physician workforce is aging, with 57% of anesthesiologists 55 yr or older. New generations, Generation Y and Z, are joining the workforce with different values than the Boomers they are replacing.8 Generation Y and Z place a great value on work–life balance. In other words, even if the total number of physicians remains the same, the total clinical capacity will be reduced due to lower work hours per clinician. This hypothesis is supported by recent evidence documenting a reduction in physician work hours over the past two decades and a trend toward unionization. Finally, noting an aging workforce, a recent article assessing selected academic practices reported anesthesiology as the highest specialty with “intent to leave” their current practice in the next 2 yrs.”1
Even though many of you feel you are underpaid (and undervalued), there is no question that anesthesiologists are amongst the highest paid professionals in America. Indeed, the high pay is one of the reasons that so many medical students want to enter the profession. But consider for a moment who pays? In the days of yore, fee for service was the primary revenue source for physician anesthesia services. No more. Currently, facility funding under writes the difference between revenue coming in and the salaries being paid. But for how much longer? And as the supply of anesthesiologists shrinks the demand for higher salaries increases, adding further stress to the system and the financial stress on institutions is simply unsustainable. (WJG) The average facility support for anesthesia services (Private or Academic) is somewhat north of $140,000 / FTE. With most health systems under significant financial distress, coupled with the increased anesthesia coverage shortages, administrators are left with the question “what are we paying for?”. More and more the response has been to directly employ the anesthesia groups and control the cost. Hence, no support for other missions such as training and research.
Academic practices are cracking and the workforce imbalances threaten the mission. What is the mission? For most academic practices the mission is a 3-legged stool (really a tricycle in my [WJG] view where the large front wheel is clinical care driving and steering the other 2 missions), defined by patient care, education and research. As hospitals and universities pay more and more for clinical care they wonder why they should be paying for non-revenue producing non-clinical time? Increasingly this time is disappearing and results in a “a series of consequences beyond increased clinical workload, forced overtime, and extended work hours. Staffing shortages create a reinforcing “education gap” feedback loop that affects resident teaching, supervision, and mentorship. As teaching physicians get busier, directly delivering clinical care, their attention to education declines. This education gap translates into poor faculty teaching scores and declining training program evaluations. Measures designed to mitigate the education gap may burden already overextended staff, decrease morale, and increase attrition rates. Education takes focused time and effort, and the current labor shortage has stressed the ability to maintain and protect academic time that is needed for high-quality education.”1 I (WJG) suspect that AI will disrupt and make more equitable and available our notion of medical training as it has in many education systems.
We wonder if academic medicine as we knew it is doomed or even resuscitatable? We face the grim reality that as we lose the academic mission, our “profession” becomes more and more a “guild” designed more to safeguard our incomes rather than our commitment to the growth and sustainability of the profession. I JC) think it is clear we have been in an era (for a while) where many faculty working in academic institutions simply choose to be clinician/teachers with no interest in other academic pursuits. A small minority actually make an effort to pursue clinical or translational research. We need to focus “non-clinical time” on that subgroup and martial resources to specifically help fund those pursuing basic science in our field – recognizing that the money to support this is very scarce. I think it would be important to point out that It is not possible for a “trade guild” to continue as a viable professional cohort. We have to insist with our administrative colleagues that research and quality improvement initiatives are not “an option”, they are a requirement. Otherwise, we will simply lose all credibility with our patients and our surgical/medical colleagues that we are fulfilling our obligations as professionals.
In tomorrow’s PAAD we will explore some possible solutions that could increase our productivity while maintaining our professional existence.
Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Abouleish AE, Pomerantz P, Peterson MD, et al. Closing the Chasm: Understanding and Addressing the Anesthesia Workforce Supply and Demand Imbalance. Anesthesiology 2024. DOI: 10.1097/aln.0000000000005052.
2. Muffly MK, Singleton M, Agarwal R, et al. The Pediatric Anesthesiology Workforce: Projecting Supply and Trends 2015-2035. Anesthesia and analgesia 2018;126(2):568-578. (In eng). DOI: 10.1213/ane.0000000000002535.
3. Nasr VG, Staffa SJ, Vener DF, et al. The Practice of Pediatric Cardiac Anesthesiology in the United States. Anesthesia and analgesia 2022;134(3):532-539. (In eng). DOI: 10.1213/ane.0000000000005859.
4. Niconchuk JA, Newton MW. Global pediatric surgery and anesthesia inequities: how do we have a global effort? Current opinion in anaesthesiology 2022;35(3):351-356. (In eng). DOI: 10.1097/aco.0000000000001122.
5. Anders G. Numb and Number: Once a Hot Specialty, Anesthesiology Cools As Insurers Scale Back ---Health-Care Workers Find Fewer Jobs, Lower Pay In Era of Cost-Cutting --- Working Harder for $100,000. The Wall Street Journal: Dow Jones & Company; 1995.
6. Giustini AJ, Sivak EL, Nasr VG, et al. Where have all the pediatric anesthesiology fellows gone in the USA? Anesthesiology fellowship trends. Paediatric anaesthesia 2024 (In eng). DOI: 10.1111/pan.14844.
7. Afonso AM, Cadwell JB, Staffa SJ, Sinskey JL, Vinson AE. U.S. Attending Anesthesiologist Burnout in the Postpandemic Era. Anesthesiology 2024;140(1):38-51. (In eng). DOI: 10.1097/aln.0000000000004784.
8. Holzer BM, Ramuz O, Minder CE, Zimmerli L. Motivation and personality factors of Generation Z high school students aspiring to study human medicine. BMC Med Educ 2022;22(1):31. (In eng). DOI: 10.1186/s12909-021-03099-4.