


Suzetrigine (pronounced suzzette-tre-gene) and the quest for the holy grail of pain therapy
Myron Yaster MD and Mark Schreiner MD

Opioids remain the gold standard for the treatment of moderate to severe pain. But it comes with a price, nausea, vomiting, constipation, somnolence, respiratory depression, tolerance, dependence and the risk of addiction and the development of opioid use disorder. Consequently, over the past 2+ decades there has been a quest of an effective, safe alternative…the holy grail of pain therapy. In today’s PAAD by Bertoch et al.1 and its accompanying editorial by Rathmell et al. 2 report that Suzetrigine, (pronounced suzzette-tre-gene) an oral, nonopioid small molecule, which selectively inhibits the voltage-gated sodium channel 1.8 (NaV1.8) may be that grail. In today’s PAAD, Dr. Mark Schreiner and I will discuss how it works and what the investigators found. But first a word from Monty Python on questing for the other, classic holy grail.
Editorial
Rathmell JP, Clark JD, Eisenach JC. Suzetrigine: First in a New Class of Nonopioid Analgesics for Acute Pain. Anesthesiology. 2025 Jun 1;142(6):989-991. doi: 10.1097/ALN.0000000000005465. Epub 2025 May 13. PMID: 40358331.
Original article
Bertoch T, D'Aunno D, McCoun J, Solanki D, Taber L, Urban J, Oswald J, Swisher MW, Tian S, Miao X, Correll DJ, Negulescu P, Bozic C, Weiner SG. Suzetrigine, a Nonopioid Na V 1.8 Inhibitor for Treatment of Moderate-to-severe Acute Pain: Two Phase 3 Randomized Clinical Trials. Anesthesiology. 2025 Jun 1;142(6):1085-1099. doi: 10.1097/ALN.0000000000005460. Epub 2025 Mar 21. PMID: 40117446; PMCID: PMC12061372.
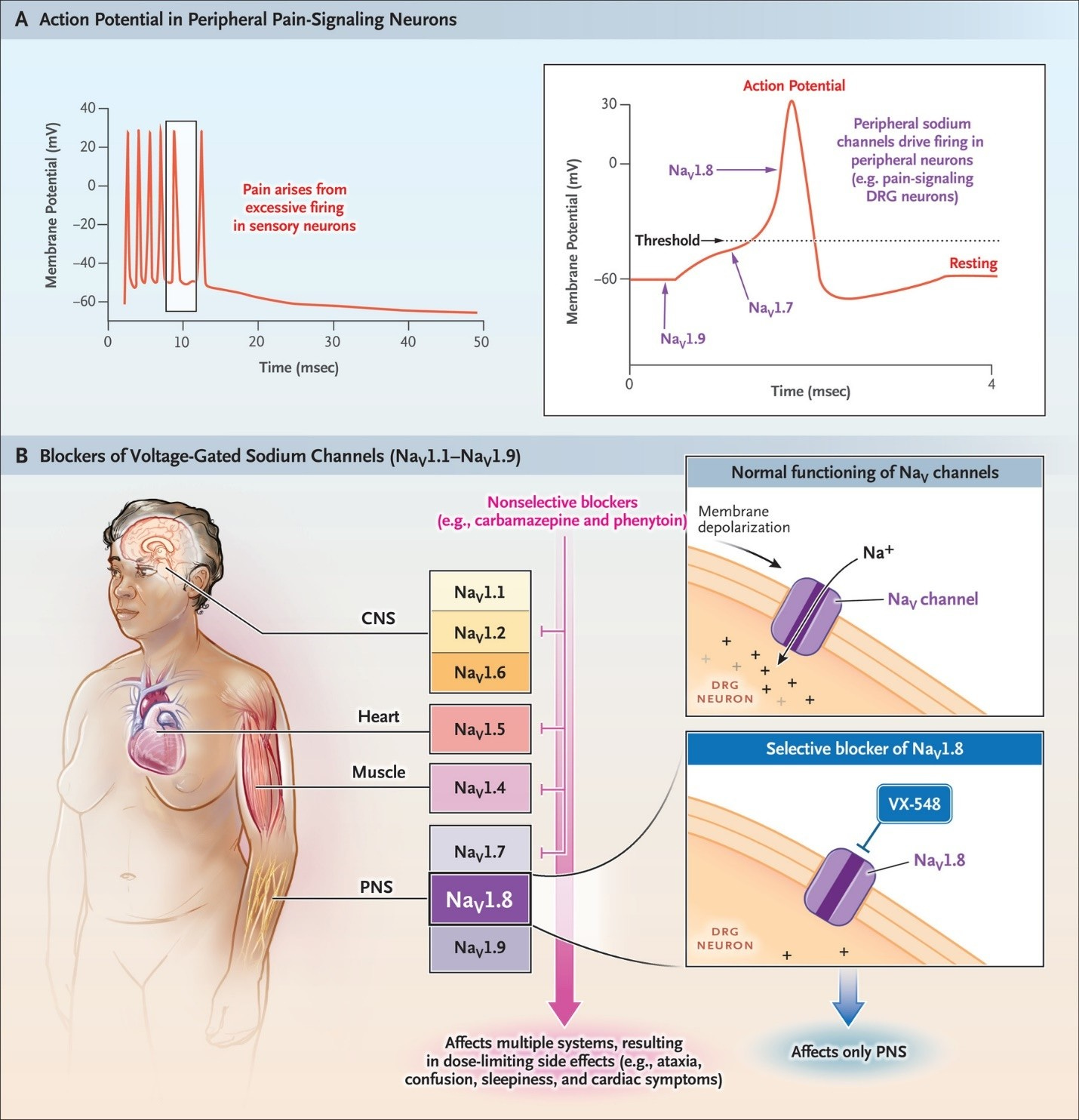
To understand how Suzetrigine (the brand name: Journavx, Vertex pharmaceuticals…pronounced jor-na-VIX NOT jor-na-VAX) works let’s think about the local anesthetics we use in our everyday practice like lidocaine or ropivacaine. Local anesthetics non-selectively suppress action potentials in all excitable tissues by blocking voltage-gated Na+ channels. In doing so, they inhibit action potentials in nociceptive fibers and so block the transmission of pain impulses. They also block transmission in the heart and in the brain (figure from NEJM articles below). Suzetrigine is novel small molecule that binds tightly to the Na V 1.8 channel with 31,000:1 selectivity over other Na V channels.3,4 This highly selective voltage-gated sodium channel 1.8 (NaV1.8) is selectively expressed in peripheral visceral and somatosensory neurons and like local anesthetics block the transmission of pain. However, because they are located only in peripheral sensory nerves and not in the central nervous system, spinal cord, nor other organs like the heart.3 they are unlikely to lead to seizures, addiction, nor inhibit cardiac automaticity leading to ventricular escape rhythms and eventually asystole. Ah! The holy grail!
We’ve discussed the basic science of voltage-gated Na+ channels in a previous PAAD (Aug 17, 2023 Peripheral Sodium Channel: the holy grail? For a deeper dive or journal club see articles from the New England J of Medicine reviewed in that PAAD.
Physiology review
Waxman, S. G. (2023). Targeting a Peripheral Sodium Channel to Treat Pain. New England Journal of Medicine, 389(5), 466-469. https://doi.org/10.1056/NEJMe2305708
Original article
Jones, J., Correll, D. J., Lechner, S. M., Jazic, I., Miao, X., Shaw, D., Simard, C., Osteen, J. D., Hare, B., Beaton, A., Bertoch, T., Buvanendran, A., Habib, A. S., Pizzi, L. J., Pollak, R. A., Weiner, S. G., Bozic, C., Neg Waxman SG. Targeting a Peripheral Sodium Channel to Treat Pain. New England Journal of Medicine. 2023;389(5):466-469. doi:10.1056/NEJMe2305708ulescu, P., & White, P. F. (2023). Selective Inhibition of NaV1.8 with VX-548 for Acute Pain. New England Journal of Medicine, 389(5), 393-405. https://doi.org/10.1056/NEJMoa2209870
Many studies that work in the laboratory do not pan out in human trials. In today’s PAAD, Bertoch et al performed a prospective, controlled, randomized trial in ADULT human subjects who underwent abdominoplasty or bunionectomy, the classic acute pain models, to evaluate suzetrigine for treatment of acute pain. This was “a two phase 3, randomized, double-blind, placebo- and active-controlled trials conducted in adults with moderate-to-severe acute pain on the verbal categorical rating scale and 4 or greater on the numeric pain rating scale after abdominoplasty (n = 1,118) or bunionectomy (n = 1,073). After surgery, participants were randomized to suzetrigine (100 mg, then 50 mg every 12 h), hydrocodone bitartrate/acetaminophen (5/325 mg every 6 h), or placebo for 48 h. The primary endpoint was time-weighted sum of the pain intensity difference in numeric pain rating scale from 0 to 48 h (SPID48) versus placebo. Key secondary endpoints were SPID48 versus hydrocodone bitartrate/acetaminophen and time to 2-point or greater reduction in numeric pain rating scale from baseline versus placebo.”2
What did they find? “The primary endpoint was achieved in both trials with suzetrigine demonstrating statistically significant and clinically meaningful reduction in pain versus placebo. The least squares mean difference in SPID48 between suzetrigine and placebo was 48.4 (95% CI, 33.6 to 63.1; P < 0.0001) after abdominoplasty and 29.3 (95% CI, 14.0 to 44.6; P = 0.0002) after bunionectomy. Neither trial achieved the first key secondary endpoint of superiority of suzetrigine versus hydrocodone bitartrate/acetaminophen on SPID48. For the second key secondary endpoint of time to 2-point or greater reduction in numeric pain rating scale, suzetrigine had a more rapid onset of clinically meaningful pain relief versus placebo after abdominoplasty (119 min vs. 480 min; nominal P < 0.0001) and bunionectomy (240 min vs. 480 min; nominal P = 0.0016). Adverse events were similar to those seen in postsurgical settings.”2
In plain English, “as compared with placebo, suzetrigine reduced moderate-to-severe acute pain over 48 h after abdominoplasty or bunionectomy.”2 Pain reduction with suzetrigine was similar but no better than hydrocodone bitartrate/acetaminophen. Suzetrigine was associated with adverse events that were mild to moderate in severity.
Like hydrocodone/acetaminophen, suzetrigine is given orally but has a slower onset of action. Thus, when it enters our anesthetic practice it will probably be given preoperatively before entering the ORs. Finally, as Rathmell et al state in their editorial, patients in the study also had access to acetaminiophen and ibuprofen. So it may work best as a component of multi-modal analgesia rather than as a single agent.
Hopefully this is but the cusp of a wave and pediatric trials will be forthcoming soon. Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Bertoch T, D'Aunno D, McCoun J, et al. Suzetrigine, a Nonopioid Na V 1.8 Inhibitor for Treatment of Moderate-to-severe Acute Pain: Two Phase 3 Randomized Clinical Trials. Anesthesiology 2025;142(6):1085–1099. (In eng). DOI: 10.1097/aln.0000000000005460.
2. Rathmell JP, Clark JD, Eisenach JC. Suzetrigine: First in a New Class of Nonopioid Analgesics for Acute Pain. Anesthesiology 2025;142(6):989–991. (In eng). DOI: 10.1097/aln.0000000000005465.
3. Han C, Huang J, Waxman SG. Sodium channel Nav1.8: Emerging links to human disease. Neurology 2016;86(5):473–83. (In eng). DOI: 10.1212/wnl.0000000000002333.
4. Osteen JD, Immani S, Tapley TL, et al. Pharmacology and Mechanism of Action of Suzetrigine, a Potent and Selective Na(V)1.8 Pain Signal Inhibitor for the Treatment of Moderate to Severe Pain. Pain and therapy 2025;14(2):655–674. (In eng). DOI: 10.1007/s40122-024-00697-0.