
Sugammadex associated anaphylaxis
Myron Yaster MD and Lynne G. Maxwell MD

Few things can be as terrifying in the OR as anaphylaxis with sudden, profound, “unexplained” and unexpected hypotension, bronchospasm, and cardiovascular collapse. Lynne and I experienced this terror frequently in the 1980s when latex allergy, a new phenomenon at the time, swept through our practices. To the list of common culprits, namely antibiotics, neuromuscular blockers, latex, chlorhexidine, and IV contrast, we can now add sugammadex. Today’s PAAD by Chia and Wolfe1 is a wonderful review that we will summarize for you in today’s PAAD. And without sounding like a broken record, if you haven’t already downloaded the Society for Pediatric Anesthesia’s Pedi Crisis app v 2 onto your phone (available in both the Apple and Android stores), do it now! You’ll need it to follow along with the PAAD. Myron Yaster MD
Original article
Chia PA, Wolfe MW. Sugammadex-Associated Anaphylaxis: Summary and Proposed Management. Anesth Analg. 2024 Aug 1;139(2):273-277. doi: 10.1213/ANE.0000000000006759. Epub 2024 Mar 6. PMID: 38446697

“Sugammadex, a modified γ cyclodextrin, was approved by the US Food and Drug Administration (FDA) in 2015 for reversal of steroidal neuromuscular blockade.2”1 “Although it has a relatively safe profile, adverse reactions such as nausea, vomiting, pain, hypotension, bradycardia, drug–drug interactions (eg, as a steroid binder, it may reduce the effectiveness of oral contraceptives), hypersensitivity, and anaphylaxis have been described.”1 The incidence of anaphylaxis is rare, ranging from 0.01% to 0.039%.1,2 However, as our sugammadex use increases, the likelihood that one of you will see it may increase concomitantly. The big concern is what to do when it happens. For most of the drugs we use in the OR that can trigger anaphylaxis, the timing occurs early or at the mid point of an anesthetic. For sugammadex, anaphylaxis will occur at the end of a case just when our monitors and airway devices are being removed and we are transferring our patients from the OR bed to transport beds.
Diagnosis and Testing: “On examination, generalized urticaria, bronchospasm or wheezing, angioedema, an increase in peak inspiratory pressure, hypotension, tachycardia, and hypoxemia are some of the signs and symptoms that can be observed during an anaphylactic reaction.”1 In the Pedicrisis app under the Dx tab this is described as hypotension, rash, and bronchospasm. Also in the app and not in the article is the differential diagnosis: bronchospasm from URI or underlying condition; fat, thrombotic, cement embolus; sepsis. The most common symptoms reported in cases of anaphylaxis after sugammadex in the literature were hypotension, erythema or rash, and bronchospasm. A recent review of 33 published cases3 found that 18% of cases required reintubation, but no case reports specified whether airway edema was present on laryngoscopy. Intubation was most likely performed because of associated hypotension and or desaturation. A series of 3 pediatric cases was recently reported, in whom rash occurred in 3, wheezing in 2, and hypotension in 1, in whom only one remained intubated (a cardiac surgery patient, whose chest was reexplored). None were reintubated.”4
Tryptase is a protease released from activated mast cells and can be elevated in cases of anaphylaxis. Tryptase levels rise within minutes of the clinical development of anaphylaxis, peak in 30 to 90 minutes, and decline with a half-life of approximately 2 hours.5 Accordingly, tryptase levels are optimally drawn within 2 hours of the suspected event. At least 1 level should be drawn 24 hours after the event, when levels have likely normalized,1 The Pedi Crisis app recommends getting a tryptase level within 3 hours, a recommendation that should probably be reconsidered.
Treatment: As with all emergencies, declare an emergency, call for help, AND OPEN THE APP! The treatment algorithm in the article is essentially the same as in the app except the app gives pediatric dosing and doesn’t discuss the unique sugammadex issues. As stated previously, because sugammadex anaphylaxis occurs at the end of the case, there are some unique considerations. “Anaphylaxis after sugammadex administration generally occurs within 5 minutes of exposure, during which time a patient may experience tracheal extubation, transfer from the procedural table, and potentially even reduction or removal of monitoring and exit from the procedural theater. If an endotracheal tube has been removed, edema may rapidly compromise the patency of the airway. Thus, it is important to recognize the signs of anaphylaxis, because complete obstruction of the airway from angioedema can make tracheal reintubation extremely challenging or impossible.
According to the most recent anesthesia advanced cardiovascular life support (ACLS) guidelines, immediate tracheal intubation or reintubation is recommended in cases of severe anaphylaxis. If muscle relaxation is required for tracheal reintubation, succinylcholine administration should be considered if not otherwise contraindicated. Further doses of an amino-steroid nondepolarizing neuromuscular blocker may both be ineffective in the presence of sugammadex and worsen anaphylaxis if the complex is the inciting allergen, and a benzylisoquinoline nondepolarizing neuromuscular blocker may be too slow if airway edema is rapidly progressing. Assistance from other providers should be sought, including providers who can establish a surgical airway, and any monitoring that has been discontinued should be promptly reestablished. Consideration should be given to establishing invasive monitoring and access for continuous blood pressure measurement and administration of indicated medications. Clinical vigilance is paramount after sugammadex administration, and prompt management and supportive treatment are required whether or not the offending agent is known.”1 Angioedema in the setting of anaphylaxis (airway edema) should not be confused with what is more commonly referred to as angioedema: histaminergic angioedema without anaphylaxis, or non-histaminergic angioedema which is caused by C1 esterase inhibitor deficiency (hereditary angioedema) or drug reactions (especially ACE inhibitors).6
The other steps in the management of anaphylaxis are well known: follow your ABCs. Give oxygen, establish a patent airway, and support the circulation with epinephrine and fluids. How much epinephrine? Again DO NOT RELY ON YOUR MEMORY for the epinephrine dose…use the app! It will provide the IV, IO and IM single dosages as well as the infusion dose. “Medical evidence supporting the role of corticosteroids and antihistamines in the acute treatment of anaphylaxis is weak, and although administration may be considered, it should not delay first-line medications.”1 Again, the pediatric dosing of methylprednisolone, diphenhydramine, albuterol, and famotidine are in the app.
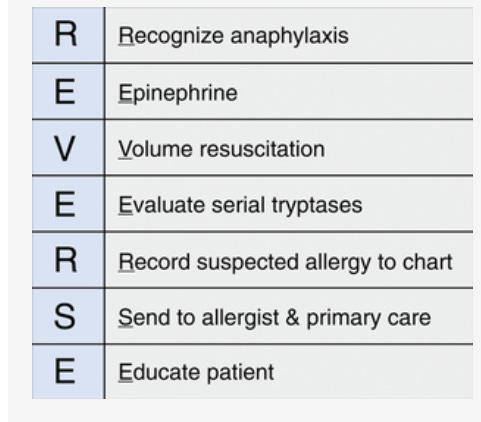
The article concludes with a mnemonic that can be used in treatment. But in reality are you going to remember the mnemonic in a crisis? We don’t think so…use the app!
We haven’t seen sugammadex anaphylaxis in our practice and we wonder if any of you have? If you have, please tell Myron about your experience and he will post your thoughts and comments in a Friday Reader response.
References
1. Chia PA, Wolfe MW. Sugammadex-Associated Anaphylaxis: Summary and Proposed Management. Anesthesia and analgesia 2024;139(2):273-277. (In eng). DOI: 10.1213/ane.0000000000006759.
2. Burbridge MA. Incidence of Anaphylaxis to Sugammadex in a Single-Center Cohort of 19,821 Patients. Anesthesia and analgesia 2021;132(1):93-97. (In eng). DOI: 10.1213/ane.0000000000004752.
3. Arslan B, Sahin T, Ozdogan H. Sugammadex and anaphylaxis: An analysis of 33 published cases. Journal of anaesthesiology, clinical pharmacology 2021;37(2):153-159. (In eng). DOI: 10.4103/joacp.JOACP_383_19.
4. Banoub R, Alalade E, Bryant J, Winch P, Tobias AJD. Allergic Reactions to Sugammadex: A Case Series and Review of the Literature. The journal of pediatric pharmacology and therapeutics : JPPT : the official journal of PPAG 2023;28(4):374-379. (In eng). DOI: 10.5863/1551-6776-28.4.374.
5. Beck SC, Wilding T, Buka RJ, Baretto RL, Huissoon AP, Krishna MT. Biomarkers in Human Anaphylaxis: A Critical Appraisal of Current Evidence and Perspectives. Front Immunol 2019;10:494. (In eng). DOI: 10.3389/fimmu.2019.00494.
6. Moellman JJ, Bernstein JA, Lindsell C, et al. A consensus parameter for the evaluation and management of angioedema in the emergency department. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine 2014;21(4):469-84. (In eng). DOI: 10.1111/acem.12341.