
Should we be using neuromuscular blockers for routine pediatric intubation?
Proshad Efune, M.D., M.S.C.S and Debra Faulk MD

Today’s PAAD by Christensen et al.[1] is a “déjà vu all over again” moment for me. Achieving optimal conditions on the first attempt at tracheal intubation remains a fundamental objective in pediatric anesthesia. Back in the day, this goal was routinely accomplished with the routine use of neuromuscular blocking agents (NMBAs). However, over the past two decades clinical practice has shifted toward avoidance of neuromuscular blockade in favor of deepening the depth of anesthesia using volatile agents or propofol–opioid (fentanyl) combinations or high-dose remifentanil. This transition was driven, in part, by concerns regarding the reversibility of neuromuscular blockade. Emerging evidence, particularly the introduction of sugammadex and quantitative monitoring now suggests that this paradigm warrants reconsideration. Myron Yaster MD
Original article
Christensen MI, Creutzburg A, Vested M, Nørskov AK, Lundstrøm LH, Afshari A. Effects of avoidance versus use of neuromuscular blocking agents for facilitation of tracheal intubation in children and infants: A systematic review with meta-analysis and trial sequential analysis. Eur J Anaesthesiol. 2026 Apr 1;43(4):335-348. doi: 10.1097/EJA.0000000000002358. Epub 2026 Feb 2. PMID: 41630605.
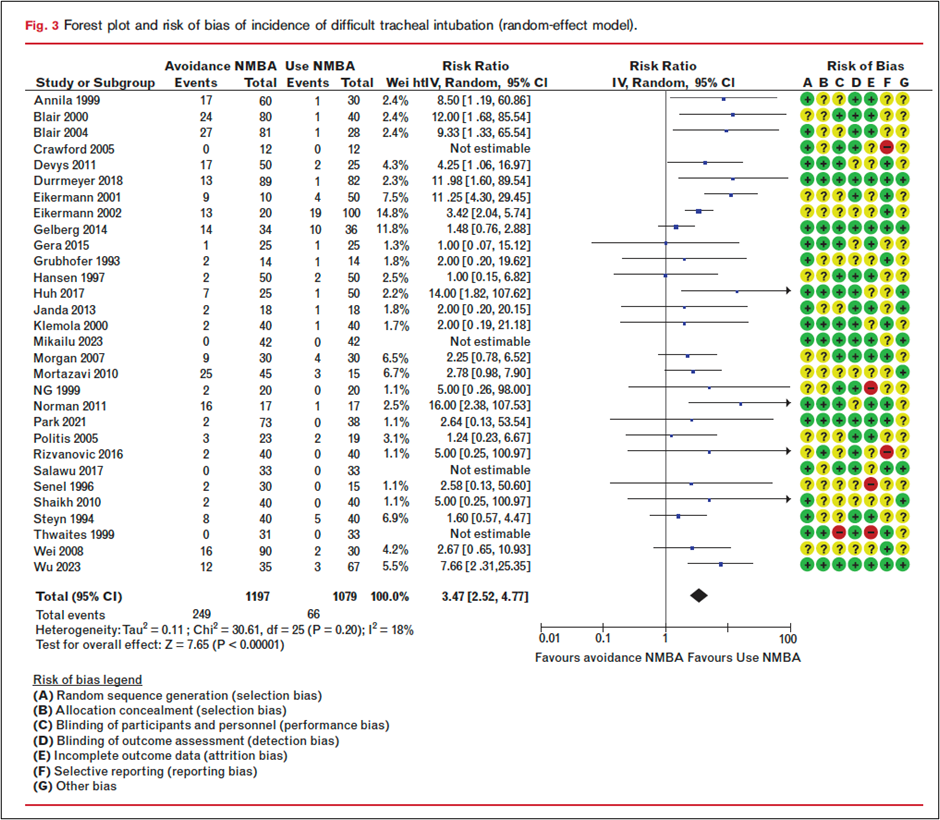
In today’s PAAD, Christensen et al.[1] performed systematic review, meta-analysis, and trial sequential analysis that provides the most comprehensive evaluation to date of neuromuscular blocking agents (NMBA) use in pediatric tracheal intubation. This work also informed the 2025 ESAIC and ESPA guidelines on neuromuscular blockade in anesthetized children.[2, 3] The authors analyzed 47 randomized controlled trials encompassing more than 3,000 patients under 18 years of age, across a range of clinical settings (operating room and neonatal intensive care unit), airway techniques (direct and video laryngoscopy), and anesthetic approaches.
The primary outcome was difficult tracheal intubation, using each study’s predefined criteria. Secondary outcomes included failed intubation and serious adverse events.
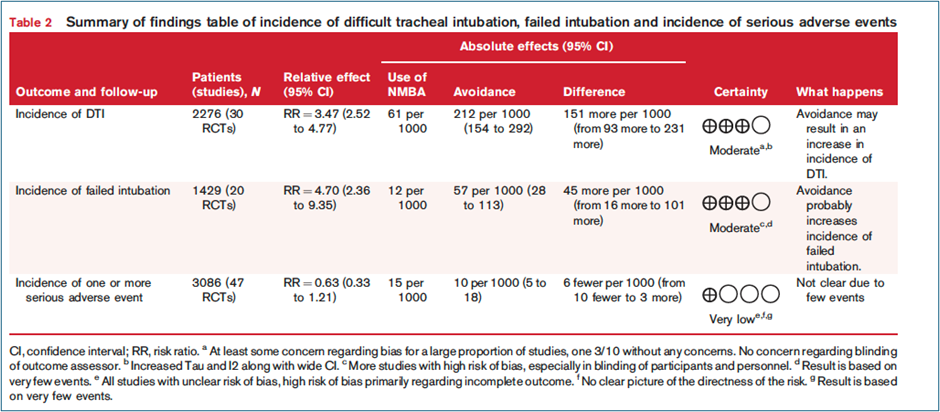
The main results of this study are not subtle. The primary outcome, difficult tracheal intubation was significantly more frequent when NMBAs were avoided. Avoiding neuromuscular blockers was associated with a greater than threefold increase in difficult tracheal intubation- 21% without NMBA vs 6% with NMBA, risk ratio 3.47 (95% CI 2.52 to 4.77), graded as moderate certainty evidence. Failed intubation was also more common without NMBA- risk ratio 4.70 (95% CI 2.36 to 9.35).
From an absolute-risk standpoint, avoiding neuromuscular blockade resulted in:
~151 additional difficult intubations per 1000 patients
~45 additional failed intubations per 1000 patients
Trial sequential analysis demonstrated that the required information size had been achieved, suggesting that these findings are robust and unlikely to change with future studies.
No significant difference in serious adverse events was observed between groups; however, these events were rare (<2%), and the certainty of this finding was low due to inconsistent reporting. Only four trials in this analysis reported SAE’s, notably chest wall rigidity.
The authors acknowledged limitations of this study, including the lack of consensus on the definition of difficult tracheal intubation and the variation in induction techniques that may lend to inadequate depth of anesthesia contributing to difficult tracheal intubation. Many trials also excluded patients with anticipated difficult airways. The predominance of American Society of Anesthesiologists (ASA) physical status I–II patients excludes consideration of more complex patients in this analysis, but may lend to the generalizability of the results in the typically healthy child presenting for anesthesia and surgery who requires endotracheal intubation.
Subgroup analyses showed no meaningful difference in the effect of NMBAs on difficult tracheal intubation between infants (<2 years) and older children, or when comparing studies with low‑ vs high‑risk‑of‑bias for the incidence of difficult tracheal intubation.
Most interestingly, post-hoc analysis stratified studies into three time periods (1993-2005, 2006-202, 2021-2025) to reflect developments in airway management including videolaryngoscopy (200’s) and the introduction of sugammadex (2010’s). The risk ratio for difficult intubation with avoidance of NMBA was above 3 across all time periods, with the highest risk ratio in the most recent trials (RR >6; 2020–2025). This suggests that advances in airway technology and novel antagonist agents have not mitigated the increased risk associated with NMBA avoidance.
Pediatric airway complications remain a leading cause of anesthesia-related morbidity. Physiologic factors including higher oxygen consumption, reduced functional residual capacity, and limited tolerance for repeated airway attempts underscore the importance of optimizing first-pass success. Collectively, current evidence supports the routine use of neuromuscular blocking agents to facilitate tracheal intubation in children. This consideration is particularly relevant in training environments, where maximizing optimal intubating conditions is critical.
Finally, as we’ve discussed in many previous PAADs, if neuromuscular blockade is used, implementation of quantitative neuromuscular monitoring is essential to ensure appropriate dosing, recovery, and patient safety, in alignment with current guideline recommendations.[2-4]
What do you do in your practice? Paralysis or deepening the anesthetic depth? Did today’s PAAD change your mind? Send your thoughts and comments to Myron (myasterster@gmail.com ) and he will post in a Friday reader response.
References
1. Christensen MI, Creutzburg A, Vested M, Nørskov AK, Lundstrøm LH, Afshari A: Effects of avoidance versus use of neuromuscular blocking agents for facilitation of tracheal intubation in children and infants: A systematic review with meta-analysis and trial sequential analysis. European journal of anaesthesiology 2026, 43(4):335–348.
2. Veyckemans F, Debouche S, Kaufmann J, Disma N, Amigoni A, Bonatti G, Christensen MI, Engelhardt T, Fuchs A, Fuchs-Buder T et al: 2025 ESAIC and ESPA Guidelines on neuromuscular block in anaesthetised children: Indications, monitoring and reversal. European journal of anaesthesiology 2026, 43(4):295–323.
3. Fuchs-Buder T, Romero CS, Lewald H, Lamperti M, Afshari A, Hristovska AM, Schmartz D, Hinkelbein J, Longrois D, Popp M et al: Peri-operative management of neuromuscular blockade: A guideline from the European Society of Anaesthesiology and Intensive Care. European journal of anaesthesiology 2023, 40(2):82–94.
4. Thilen SR, Weigel WA, Todd MM, Dutton RP, Lien CA, Grant SA, Szokol JW, Eriksson LI, Yaster M, Grant MD et al: 2023 American Society of Anesthesiologists Practice Guidelines for Monitoring and Antagonism of Neuromuscular Blockade: A Report by the American Society of Anesthesiologists Task Force on Neuromuscular Blockade. Anesthesiology 2023, 138(1):13–41.