
Rescue Rx for PONV
Katherine S. Klockau PharmD, Myron Yaster MD, and Melissa Brooks Peterson MD

Although I often feel the need for antiemetic therapy when watching the evening news (and besides me, does anyone else actually watch the evening news anymore?) Looking at the commercials, it appears that only people with type 2 diabetes or those who suffer from some form of psoriasis or small cell carcinomas are their core audiences.
As pediatric anesthesiologists, I think we’ve pretty much figured out how to prophylax for postoperative nausea and vomiting (PONV) using IV ondansetron and IV dexamethasone administered during the anesthetic. However, the conundrum of what to do in the setting of “failed prophylaxis” is not so clear. Today’s PAAD is a review of rescue therapies for PONV primarily in adult patients. In fact, the authors barely mention how to do this for pediatric patients. I decided to ask our team to review it from the lens of pediatric anesthesiologists. Unfortunately, much to my chagrin, I discovered that many of the oral drugs we routinely use for prophylaxis and/or rescue are not labeled for use in pediatric PONV by the U.S. FDA, including – gasp – oral ondansetron. (Oral ondansetron is indicated for use in pediatric induced chemotherapy and in adult PONV but not pediatric PONV. IV ondansetron is FDA labeled for pediatric PONV). Why pediatric drug labeling remains an issue in 2022 is really a scandal and hopefully some of you will comment on this issue in a reader response. I’ve asked Kate Klockau, a PharmD at the Children’s Hospital Colorado, to assist particularly on FDA labeling. Myron Yaster MD
Review article
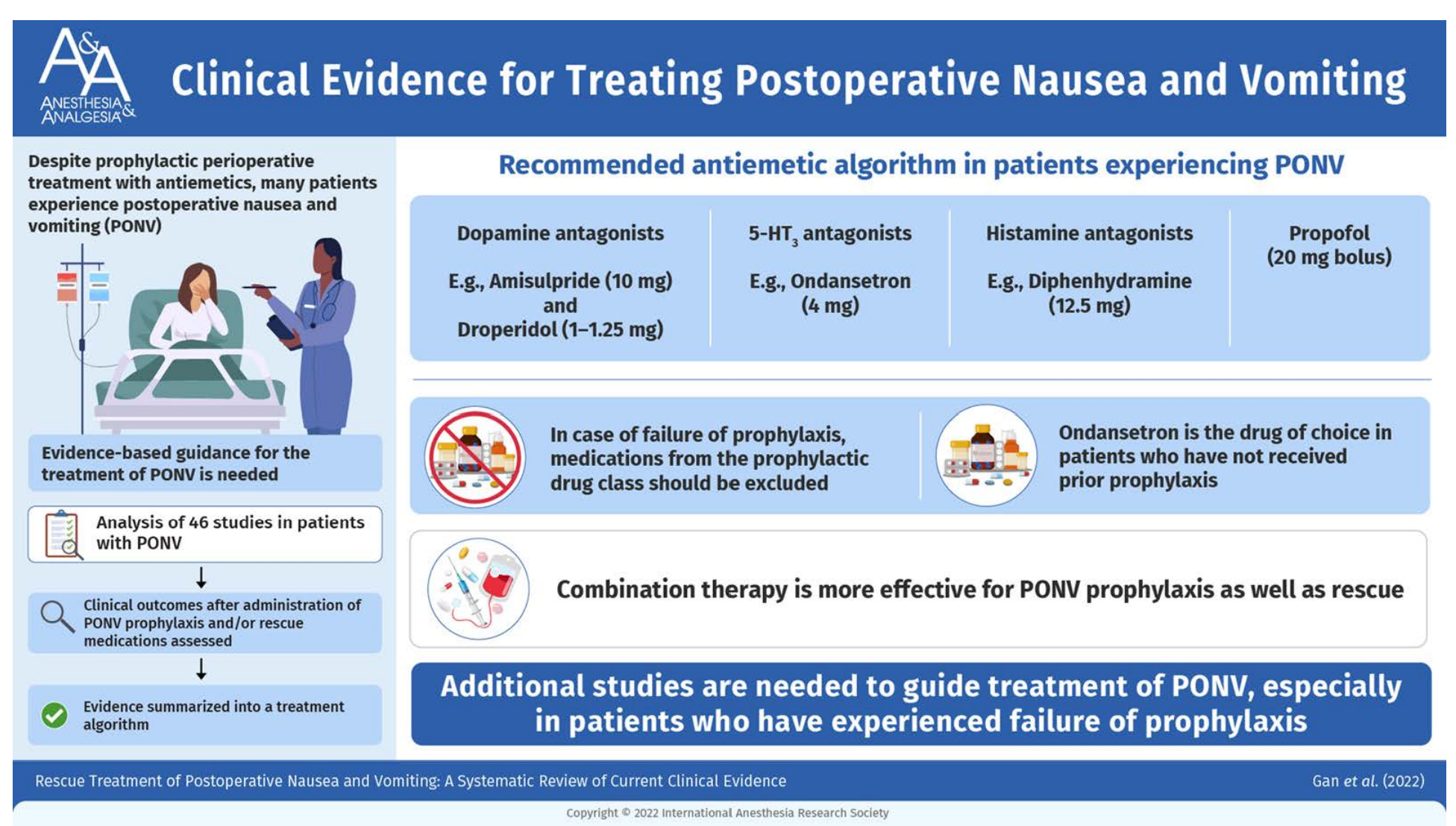
Gan TJ, Jin Z, Meyer TA. Rescue Treatment of Postoperative Nausea and Vomiting: A Systematic Review of Current Clinical Evidence. Anesth Analg. 2022 Nov 1;135(5):986-1000. PMID: 36048730
Essentially, there are 5 classes of drugs used to treat PONV.
5-Hydroxytryptamine Antagonists including ondansetron, granisetron, dolasetron, tropisetron, and palonosetron.
Dopamine Antagonists including droperidol, haloperidol, and metoclopramide.
Anti-histamines including diphenhydramine and promethazine
Neurokinin-1 Antagonists including aprepitant, rolapitant, casopitant, fosaprepitant, netupitant, and maropitant
Anti-cholinergics including scopolamine
In the PACU a small dose of IV propofol may be helpful. Non-pharmacologic methods such aromatherapy with natural essential oils or isopropyl alcohol have been reported to be almost as effective as ondansetron in the treatment of PONV.1, 2
If patients fail one class of drug for PONV, adding a second drug from a different class is more effective than giving another dose of the original antiemetic drug or another drug from the same class of anti-emetics. For example, if ondansetron was the original drug and it failed, a second dose of ondansetron or another drug from the same 5-Hydroxytryptamine antagonist family like dolasetron will often be ineffective. (Because of pharmacogenetic differences in metabolism, some patients who fail on ondansetron may benefit from the 5-HT antagonist granisetron.3) Giving a drug from the dopamine antagonist family like droperidol or metoclopramide or from the anti-histamine family like promethazine or diphenhydramine will probably be more effective. Which one to choose will be based on oral bioavailability or side effect profiles like sedation or psychomimetic effects. In reality, no one uses droperidol or metoclopramide any more. Another rescue therapy to consider is eliminating or alternating opioids from the analgesic regimen. It has been our experience that the real culprit in “PONV” especially nausea and vomiting that onsets several hours after surgery and anesthesia are the opioids used in pain management.
Ok, sounds simple enough right? I (MY) asked Kate Klockau to do a formal review of which of the oral anti-emetics is labeled for PONV by the FDA and this is what she found. There are actually very few! Oral agents she reviewed include aprepitant, diphenhydramine, metoclopramide, ondansetron, and promethazine. Oral promethazine is technically FDA labeled for PONV in pediatrics, but oral ondansetron isn’t! However, we all know that oral ondansetron in pediatrics is the gold standard and oral promethazine is almost never used in pediatric PONV! (side note: you can tell if something is “FDA labeled” by reviewing the dosing printed in the package insert itself. Package inserts can be accessed on the website www.dailymed.nlm.nih.gov or on the drug manufacturer’s website.) Further, there is a black box warning about the use of promethazine in children in less than 2. Oral diphenhydramine is labeled for use in children but only for runny nose, sneezing and itchy eyes and nose but carries no pediatric labeling for a PONV indication. Oral aprepitant is only indicated for PONV in adults. Kate and Mel report it is available at the Children’s Hospital Colorado. I (MY) am curious if any of you are using oral aprepitant either for rescue or as an initial antiemetic preoperatively? If you have experience with the oral form of this drug please send me (MY) a note with some details of your experience and I’ll post in a reader response. Finally, ondansetron in its many formulations (oral solution, tablets, rapidly disintegrating tablets) is indicated for nausea and vomiting in pediatric cancer patients but not for pediatric PONV. Similarly, IV metoclopramide has some pediatric indications but not for PONV.
There is much to say and has been said about FDA labeling and continued insufficient pediatric labeling. Frequent PAAD contributors Dr. Lynne Maxwell, Dr. Charlie Cote, and Dr. Mark Schreiner have railed about this for decades. “The absence of labeling for a specific age group or for a specific disorder does not necessarily mean that the drug’s use is improper for that age or disorder. Rather, it only means that the evidence required by law to allow inclusion in the label has not been approved by the FDA. Additionally, in no way does a lack of labeling signify that therapy is unsupported by clinical experience or data in children. Instead, it specifically means that evidence for drug efficacy and safety in the pediatric population has not been submitted to FDA for review or has not met the regulatory standards of “substantial evidence” for FDA approval. In contrast to the absence of pediatric-specific information on some medications, other drug labels contain statements such as ‘the safety and efficacy in pediatric patients have not been established,’ and explicit evidence-based warnings and contraindications are included on the label where indicated. Understanding the distinction between the lack of FDA approval for a particular use or dosing regimen in the former case versus explicit warnings or contraindications against use in the latter is essential for the pediatric practitioner.”4
We are curious as to what oral anti-emetics you use for PONV rescue and how you handle the lack of labeling indication in your practice. Send Myron an email and he will post in a reader response (myasterster@gmail.com).
References
1. Gan TJ, Jin Z, Meyer TA. Rescue Treatment of Postoperative Nausea and Vomiting: A Systematic Review of Current Clinical Evidence. Anesthesia and analgesia. Nov 1 2022;135(5):986-1000. doi:10.1213/ane.0000000000006126
2. Hunt R, Dienemann J, Norton HJ, et al. Aromatherapy as treatment for postoperative nausea: a randomized trial. Anesthesia and analgesia. Sep 2013;117(3):597-604. doi:10.1213/ANE.0b013e31824a0b1c
3. Jacobs SS, Dome JS, Gai J, et al. Pharmacogenetic and clinical predictors of ondansetron failure in a diverse pediatric oncology population. Supportive Care in Cancer. 2022/04/01 2022;30(4):3513-3520. doi:10.1007/s00520-022-06818-9
4. Frattarelli DA, Galinkin JL, Green TP, et al. Off-label use of drugs in children. Pediatrics. Mar 2014;133(3):563-7. doi:10.1542/peds.2013-4060