
Remembering the Classics: When Old is New - Flushing of Axillary Arterial Lines
Barry D. Kussman, MBBCh, SM, FFA(SA) and Shawn Jackson, MD, PhD

The risk of retrograde embolization of air or thrombus into the central arterial circulation when flushing arterial lines has been known for over 50 years.1 After arterial blood sampling, it is routine to flush the arterial line and its stopcocks and tubing to clear the line of debris, residual blood and clot, as well as air to prevent micro emboli and line clotting and thereby maintain catheter patency and function. Techniques for flushing include a bolus delivered by a hand-held syringe or initiating a continuous infusion (+/- heparin) by an electronic syringe pump or by flushing from a pressurized bag flush system. Physical factors associated with flushing that predispose to retrograde flow into the aorta include volume, duration/velocity, flushing pressure, systemic arterial pressure, cannula size, and proximity to the aortic arch. A recently published PAAD (April 28, 2025) on the use of axillary arterial lines generated a lot of attention and reader responses concerning the “how tos” of flushing arterial lines and the how tos of minizing the risk of retrograde embolization, given the proximity of the axillary and even radial artery to the cerebral circulation.
I asked Dr. Barry Kussman MBBCh, SM, FFA(SA) a pediatric cardiac anesthesiologist at Boston Children’s Hospital to participate. For those of you who don’t know him, after receiving his medical training in South Africa, he completed fellowships in pediatric anesthesia and cardiac anesthesia at Boston Children’s Hospital and the Beth Israel Hospital, respectively. His clinical focus is the perioperative care of infants, children, and adults with congenital heart disease. His research interests include neuromonitoring during cardiac surgery and measurement of pain in patients under general anesthesia. He recently graduated with a Master of Science in Bioethics from Harvard Medical School.
Original article
Lowenstein E, Little JW 3rd, Lo HH. Prevention of cerebral embolization from flushing radial-artery cannulas. N Engl J Med. 1971 Dec 16;285(25):1414-5. doi: 10.1056/NEJM197112162852506. PMID: 5121208.
Original article
Edmonds JF, Barker GA, Conn AW. Current concepts in cardiovascular monitoring in children. Crit Care Med. 1980 Oct;8(10):548-53. doi: 10.1097/00003246-198010000-00004. PMID: 7418415.
Pediatric studies to date have not examined retrograde embolization with axillary arterial catheters but have evaluated this issue with radial artery catheters. Edmonds et al.2 repeated the radial artery study by Lowenstein et al.1 in 12 children ranging in age from 5 months to 18 years and crown to heel height from 50-170 cm2. They found that the volume of flush solution necessary to produce retrograde flow into the central circulation was 0.3-0.5 mL, and like the Lowenstein study there was a correlation between patient height and the volume of flush solution (r = 0.98). Butt et al.3 studied radial artery flushing in newborn infants using ultrasound and demonstrated microbubbles in the aortic arch and left common carotid artery when 0.5 mL or 1 mL was flushed over 1 second, but not if either volume was flushed over 5 seconds with a “slow steady push”. The study by Weiss et al.4 was commented on in the April 30, 2025, PAAD, but is worth repeating. In 9 of the 16 patients (range 1-105 days, median 22 days; range 2.5-4.5 kg), microbubbles were detected in t he common carotid artery with both a 1.5-2 mL syringe pump bolus given over 2 seconds and with a bag pump pressure of 200-300 mmHg over 2 seconds.4 In all patients, emboli were detected in the subclavian artery with syringe pump boluses of 0.5-1.5 mL and at 100-200 mmHg bag pump pressure.
Murphy et al.5,6 performed two studies in adults. Their later study (n=100; age 70 ± 13 years [mean ± SD]) utilized duplex ultrasonography of the brachial and axillary arteries to determine whether retrograde arterial flow occurred with manual flushing and flush valve opening of the radial artery5. After 10 mL of saline and blood were withdrawn into a syringe within the arterial-flushing system, clinicians were instructed to compress the plunger on the syringe at a rate that reflected their standard practice. Subsequently, a second 10 mL bolus was given over 10 seconds via a bag pump system with a pressure of 300 mmHg. Retrograde flow was observed much more commonly with manual flushing (P < 0.001), and the probability of retrograde flow was related to the manual radial arterial flush duration (P < 0.001). The duration of manual flush was the only factor differentiating the presence or absence of retrograde flow. Evidence of retrograde flow in the proximal axillary artery was only observed when manual flushing was at a rate faster than 1 mL/s i.e., 0/48 patients had retrograde flow when the 10 mL was flushed over 9s or greater). The findings of this study were surprising to the investigators because in their earlier study with similar methodology no microemboli were detected in the aortic arch or carotid arteries when flushing 10 mL of saline and blood over 4-20 s (maximum rate of 2.5 ml/s).6 All the above studies were limited by lack of evaluation of the vertebral arteries.
Given the proximity of the axillary artery to the cerebral circulation, adopting cautious flushing techniques becomes integral to patient safety (Figure). Extrapolating from these studies to the flushing of axillary arterial lines suggests the following as reasonable precautions pending studies to the contrary: (1) flush volumes should be minimized, ideally as low as 1 mL when possible. However, unless the flush volume is administered via a stopcock very close to the arterial cannula, we acknowledge that larger volumes may be required for adequate line maintenance; (2) the velocity of the flush should not exceed 1 mL/s and more ideally, should be 0.5 mL/s. This speed, in practice, feels profoundly slow, but is likely the most important factor to reduce embolization; and (3) maintain a vertical orientation of the syringe (with the plunger at the top) to further reduce embolization risk. We feel that this simple aspect of our care is worth highlighting, especially to our trainees and rotators who may have limited pediatric exposure (as well as clinicians in the ICU). By emphasizing these best practices, we can enhance their awareness and competency, ultimately improving outcomes for our young patients. As this field continues to evolve, staying informed and vigilant about these procedures will remain a cornerstone of effective pediatric anesthetic care.
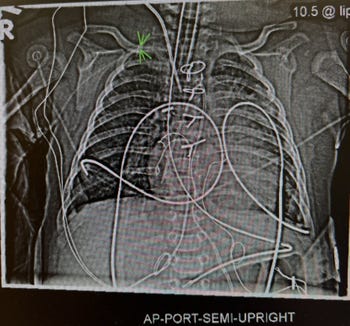
Figure Legend: CXR in an infant with a right axillary arterial catheter size 24G and length 5 cm. Green arrows indicate tip of the catheter very close to the subclavian artery.
Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Lowenstein E, Little JW, 3rd, Lo HH. Prevention of cerebral embolization from flushing radial-artery cannulas. The New England journal of medicine 1971;285(25):1414–5. (In eng). DOI: 10.1056/nejm197112162852506.
2. Edmonds JF, Barker GA, Conn AW. Current concepts in cardiovascular monitoring in children. Critical care medicine 1980;8(10):548–53. (In eng). DOI: 10.1097/00003246-198010000-00004.
3. Butt WW, Gow R, Whyte H, Smallhorn J, Koren G. Complications resulting from use of arterial catheters: retrograde flow and rapid elevation in blood pressure. Pediatrics 1985;76(2):250–4. (In eng).
4. Weiss M, Balmer C, Cornelius A, Frey B, Bauersfeld U, Baenziger O. Arterial fast bolus flush systems used routinely in neonates and infants cause retrograde embolization of flush solution into the central arterial and cerebral circulation. Canadian journal of anaesthesia = Journal canadien d'anesthesie 2003;50(4):386–91. (In eng fre). DOI: 10.1007/bf03021037.
5. Murphy GS, Szokol JW, Marymont JH, Avram MJ, Vender JS, Kubasiak J. Retrograde blood flow in the brachial and axillary arteries during routine radial arterial catheter flushing. Anesthesiology 2006;105(3):492–7. (In eng). DOI: 10.1097/00000542-200609000-00012.
6. Murphy GS, Szokol JW, Marymont JH, Avram MJ, Vender JS. Retrograde air embolization during routine radial artery catheter flushing in adult cardiac surgical patients: an ultrasound study. Anesthesiology 2004;101(3):614–9. (In eng). DOI: 10.1097/00000542-200409000-00009.