
Remembering the classics: Platelets and Massive Blood Loss
Charles Coté MD

I recently had the opportunity of reading and reviewing the 3d edition of (Ron) Litman’s Basics of Pediatric Anesthesia for the journal Anesthesiology. I’ll have more to say about that when the review is accepted and published by the journal. Admittedly this was the first time I read a textbook from cover to cover since I studied for my own written Boards several decades ago. It afforded me the opportunity to rediscover classic articles that we haven’t covered in previous PAADs. One topic I was particularly looking for was the perioperative management of pediatric burn patients. There are several recurrent themes in the perioperative management of pediatric burn patients including: how to assess the extent of the burn, how to monitor when there isn’t a hell of a lot of real estate to attach monitors, blood and fluid management, hypermetabolism, drugs to use and not use for neuromuscular blockade, temperature and pain management to name just a few. In looking through the reference list, I found several classic and foundational articles and not surprisingly, some were by a frequent PAAD contributor, Dr, Charles (Charlie) Coté.1 I asked him to look thru his CV to find one or two of his most important papers on this topic as “a remembering the classics” for the PAAD readership. Today he will review his original article on serial platelet counts following massive blood transfusions, next month he will review his classic paper on Citrate Toxicity and Fresh Frozen Plasma. Myron Yaster MD
Original article
Coté CJ, Liu LM, Szyfelbein SK, Goudsouzian NG, Daniels AL. Changes in serial platelet counts following massive blood transfusion in pediatric patients. Anesthesiology. 1985 Feb;62(2):197-201. doi: 10.1097/00000542-198502000-00024. PMID: 3970376.
When I first started at the Massachusetts General Hospital, I had no prior experience with the care of children with burns and it was common for them to lose 1-3 blood volumes with each trip to the operating room. Since they all were fully monitored with arterial and central venous lines this provided a perfect opportunity to examine what happens to platelet counts.
After IRB approval we then prospectively studied a convenience sample of children with and without burn injuries who underwent procedures involving the loss of one or more blood volumes. We estimated each blood volume loss as equivalent to transfusion of blood products equivalent to their calculated blood volume while maintaining a constant central venous pressure.
After 26 patients were studied we examined our data2 and compared it with data that Dr. Ron Miller had gathered during his time in Vietnam.3 He reported the reduction in platelet counts per 10 units of whole blood transfused (ideal 70 kg man = 70 mL/kg = a blood volume of ~10 units of whole blood). He found that the reduction in platelet counts did not follow strict predictions for dilution suggesting mobilization of platelets at a time of stress.
For our patients we estimated the blood volume to be 75 mL/kg for those < 1 year and for all others 70 mL/kg. Transfusions were with packed red blood cells, FFP, 5% albumin and lactated Ringers as indicated. We observed the surgical field for signs of abnormal bleeding or oozing; when both the attending anesthesiologist and the surgeon agreed we made note of that time and the corresponding platelet counts. All children were hemodynamically stable throughout and did not demonstrate hypoxia, acidosis, or hypovolemic hypotension. Our cohort had ages 1-17 years (mean 5.9 years) and weight 10 – 70 kg (mean 25 kg) and consisted of 17 burn patients, 6 spinal instrumentation, one Wilm’s tumor, one neuroblastoma, and one radical pancreatectomy. All lost at least one blood volume, 12 lost two blood volumes, 4 lost three blood volumes, 2 lost four blood volumes and 1 lost five blood volumes. Seven children received platelets (0.3 units/kg for 6 and 0.8 units/kg for 1). Three received platelets because their counts had decreased to 64,000 -142, 000/mm3 and considerably more blood loss was anticipated (2 burn patients and 1 non-burn patient). Four patients developed signs of abnormal bleeding with platelet counts of 34,000, 46,000, 46,000 and 92,000/mm3. The patient with the platelet count of 92,000/ mm3 was a spinal instrumentation patient who had slipped off support with a rolled towel compressing the abdomen; when it was removed all abnormal bleeding stopped! The remaining 3 patients with low platelet counts had normal PTs and PTTs and the abnormal bleeding stopped with platelet transfusions; the rise in platelet count 1 hour after transfusion ranged from +82,000/mm3 to -20,000/mm3 in a patient with ongoing blood loss. The abnormal bleeding stopped immediately in the 3 patients with the lowest platelet counts.
We plotted Ron Miller’s data from 21 young adult males with our data from 26 pediatric patients using blood volumes transfused rather than units of blood transfused and found that our data was virtually superimposable on those of Miller (Figure 1).

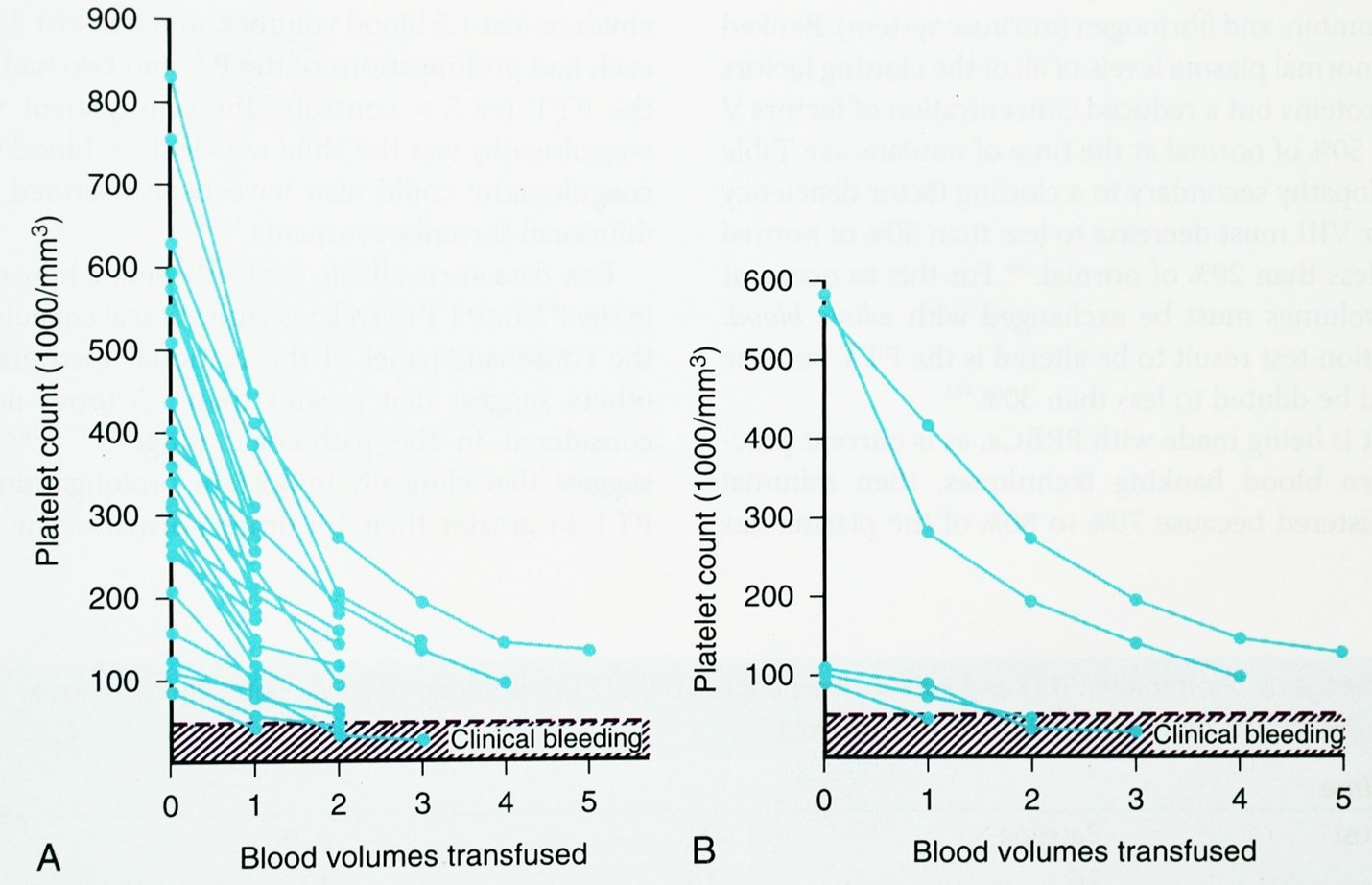
Thus, using blood volumes transfused rather than units of blood products transfused is the most reliable way of estimating when platelets are likely to be required assuming normal platelet function from the beginning of the case (these data would not apply to children undergoing cardiac bypass). More importantly we found that the threshold for abnormal bleeding in otherwise healthy children seems to be approximately < 50, 000/mm3 (Figure 2A). Figure 2A plots the serial changes in platelet count vs blood volumes lost for all 26 children and figure 2B plots 5 selected patients. Note that the three children who began with low platelet counts required platelet transfusions between 1 and 2 blood volumes but two children who lost 4-5 blood volumes never required platelets because their starting count were so elevated.
Conclusions: 1) the fall in platelet counts during massive blood loss in children is similar to those observed in adults when weight normalized 2) a low baseline platelet count is predictive of the need for platelets when blood loss reaches ~1 blood volume but for patients with a very high baseline platelet count there may be no need for a platelet transfusion despite blood losses of many blood volumes.
Or data, although based on a relatively small cohort, suggest that one can estimate a loss of ~ 40 % of the baseline platelet count after one blood volume lost and replaced, another 20 % with the second blood volume and a further 10% at three blood volumes lost and replaced. Thus, after a loss of 3 blood volumes the patient would likely still have approximately 30 % of their baseline platelet counts. Knowing where you start will inform you where you are headed! Fortunately with surgeons more tuned into reducing blood loss and improved blood conservation techniques these types of losses are less common for elective procedures but certainly may well apply to trauma patients.
Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Firth PG, Mai CL. The evolution of pediatric sedation and anesthesia patient safety: An interview with Dr Charles J. "Charlie" Coté. Paediatric anaesthesia 2020;30(11):1183-1190. (In eng). DOI: 10.1111/pan.13999.
2. Cote CJ, Liu LM, Szyfelbein SK, Goudsouzian NG, Daniels AL. Changes in serial platelet counts following massive blood transfusion in pediatric patients. Anesthesiology 1985;62(2):197-201.
3. Miller RD, Robbins TO, Tong MJ, Barton SL. Coagulation defects associated with massive blood transfusions. Annals of surgery 1971;174(5):794-801. (In eng). DOI: 10.1097/00000658-197111000-00010.