
Remembering the classics: Managing Apparatus Dead Space in the Anesthetized Infant
Jeffrey M. Feldman MD MSEd and Britta S von Ungern-Sternberg MD, PhD

Today’s remembering the classics1 is the first of several papers we will be reviewing over the next few months that deal with ventilation and ventilator mechanics that affect your practice of pediatric anesthesia on a daily basis. The reviewers, Drs. Jeff Feldman and Britta von Ungern-Sternberg are leaders in this field and have written extensively about these issues. Dr. Feldman is a Professor of Clinical Anesthesiology, Children’s Hospital of Philadelphia, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA. Dr. von Ungern-Sternberg is a Professor and Chair, Paediatric Anaesthesia, Division of Emergency Medicine, Anaesthesia and Pain Medicine, The University of Western Australia, Perth, Australia, Department of Anaesthesia and Pain Medicine, Perth Children’s Hospital, Perth, Australia, Institute for Paediatric Perioperative Excellence, The University of Western Australia, Perth, Australia, Perioperative Medicine Team, Perioperative Care Program, Telethon Kids Institute, Perth, Australia.
Original article
Pearsall MF, Feldman JM. When does apparatus dead space matter for the pediatric patient? Anesth Analg. 2014 Apr;118(4):776-80. doi: 10.1213/ANE.0000000000000148. PMID: 24651232.
During anesthesia, it can be challenging to achieve the goals of side-stream gas sampling and humidification of the airway while minimizing apparatus dead space, especially in small patients. Apparatus dead space consists of the internal volume of components added to the breathing system between the y-piece and the endotracheal tube. The impact of apparatus dead space in the breathing circuit is a problem when ventilating small patients that is “hiding in plain sight.” When apparatus dead space is greater than desired, the result will be hypercarbia, which may go unrecognized since the end-tidal CO2 measurement will not reflect the elevated PaCO2.2
In this issue of the PAAD, we revisit prior literature on the relationship between apparatus dead space and the effectiveness of mechanical ventilation in pediatric patients. Guidance for managing apparatus dead space according to patient size is reviewed, including recent changes to the supply of low dead space endotracheal tube connectors.
In today’s classic paper, Pearsall and Feldman measured and reported the dead space of some commonly used connectors that impact apparatus dead space in the anesthesia circuit.1 These connectors are used to sample airway gases for analysis, provide heat and moisture exchange (HME), and make the circuit connection to the endotracheal tube more convenient. In addition, the authors developed a simple one-compartment model to estimate the impact of apparatus dead space on alveolar CO2 (PACO2) by patient size. The model demonstrates that there is an exponential rise in PACO2 if minute ventilation is unchanged as dead space increases. An earlier in vivo study of the impact of adding a large HME to the breathing circuit showed results similar to those estimated by the model in small patients.3 Not unexpectedly, these references show that increasing apparatus dead space has a more significant impact on PACO2 in smaller patients than in larger patients. (Figure 1).

Legend: Family of plots estimating the impact of increasing apparatus dead space on PACO2 by patient size when minute ventilation remains constant.1
The model is also used to show it may be possible to offset the increase in PACO2 to some degree by increasing minute ventilation, but there are disadvantages to this approach. The primary disadvantage is exposing the lung to greater energy than would otherwise be needed, potentially increasing the risk of ventilator-induced lung injury, especially in vulnerable populations that have underlying lung disease.4 Further, if apparatus dead space becomes too great, CO2 cannot be controlled reliably by increasing minute ventilation. Whereas many healthy patients will tolerate hypercarbia quite reasonably, that is not true for all patients. Patients with a reactive pulmonary circulation at risk for pulmonary hypertension as well as those with intracranial pathology require careful control of PaCO2. Given the challenges of mechanical ventilation when caring for pediatric patients with specific pathology or undergoing complex procedures, managing apparatus dead space well removes one consideration when it becomes challenging to achieve good gas exchange. A more recent publication by King and Feldman provides further guidance for managing apparatus dead space effectively for all sizes of patients.5
In this paper, King and Feldman briefly review the physiology of dead space, summarizing the relationship between patient size and the impact of apparatus dead space on ventilation, specifically elimination of CO2.5 The authors specifically draw attention to the need to sample gases for analysis during anesthesia care, maintain humidity in the lungs and the potential dead space penalty imposed by devices used to achieve those goals. Using a rule of thumb to limit apparatus dead space to one-third of the desired tidal volume, guidance is provided for managing apparatus dead space by patient size. Three categories of recommendations are provided for minimal dead space (<5 Kg), low dead space (5-15 Kg), and normal dead space (> 15 Kg). (Figure 2).
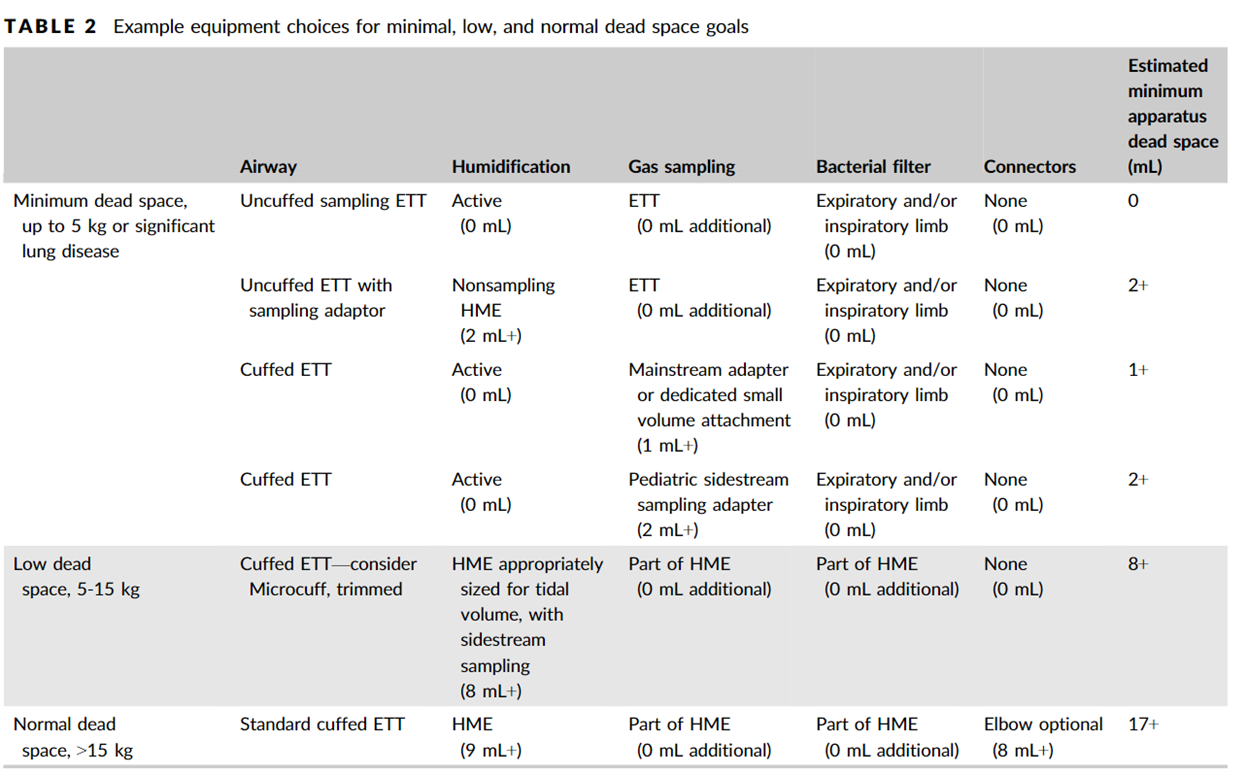
Legend: Guidance for managing breathing circuit devices commonly used during anesthesia that impact apparatus dead space for different size patients.5
Our tiniest patients are typically the most vulnerable and require unique solutions. This is certainly true when managing apparatus dead space for patients who weigh less than 5 kg. Specifically, the best solution recommended by King and Feldman for these small patients has been to exchange the endotracheal tube connector with a low dead space version with an integrated gas sampling port. Combining this connector with a small dead space dedicated heat and moisture exchanger achieves the goals of gas sampling and humidification with minimal added dead space. (Figure 3) When using these devices, capnography becomes as reliable as possible for estimating PaCO2, and if hypercarbia ensues, attention can be directed to ensuring minute ventilation is adequate without concern for the impact of apparatus dead space.

Legend: Example of 15 mm endotracheal tube connector with gas sampling port that can be used without increasing apparatus dead space. (Smith’s Medical – No longer manufactured)
Supply Chain and the Small Dead Space Connector
The unique endotracheal tube connector in Figure 3 was originally manufactured by Portex, which was acquired by Smith’s Medical and ultimately became part of ICU Medical. Unfortunately it is no longer manufactured or available as a standalone product. Rather, it is now manufactured and packaged with an appropriately sized uncuffed endotracheal tube.(figure 4).
Legend: Smiths Medical Endotracheal Tube Murphy with Low Dead Space Sideport Connector
Pediatric devices are always susceptible to the orphan device problem when the potential market size is too small to justify the expense of manufacturing and distributing a medical device. While it appeared that the low dead space connector had fallen prey to this problem, fortunately, the device was repackaged to include an uncuffed endotracheal tube as well. While it may seem more convenient to have the connector and tube together, we believe it is more convenient and environmentally friendly to have them packaged separately. It is not uncommon to trial different endotracheal tube sizes in a small patient and traditionally, we were able to reserve the low dead space connector until the proper size tube was determined. It is also our preference to use cuffed endotracheal tubes as they provide the most flexibility for ensuring reliable ventilation without leaks, especially in the dynamic environment of the operating room. Also, for patients who remained intubated after the procedure, the gas sampling connector is removed, and the original connector replaced to avoid a source of an unidentified leak in the ICU setting. Patients who come to the OR from NICU already intubated could receive a unique connector in theatre, without the need of a new tube as well. While we are pleased to be able to have a continued source of these connectors, it is quite likely that the endotracheal tube supplied with the connector will go unused.
The low dead space endotracheal tube connector, especially for patients under 5 kg, remains a convenient low-cost solution to sampling respiratory gases without increasing apparatus dead space. Fortunately, the device solution remains available, albeit only as part of a more wasteful package.
PS: from Myron: I found the supply chain and lack of availability of the low profile endotracheal tube adaptor really disturbing. I understand it was a business decision by a company, Smiths medical, that in the past was very responsive to the pediatric anesthesia and critical care community. I wonder if as a community we can band together to reverse this decision. Send your thoughts and comments to me I will post in a Friday reader response.
References
1. Pearsall MF, Feldman JM. When does apparatus dead space matter for the pediatric patient? Anesthesia and analgesia 2014;118(4):776-80. (In eng). DOI: 10.1213/ane.0000000000000148.
2. Humphreys S, Schibler A, von Ungern-Sternberg BS. Carbon dioxide monitoring in children-A narrative review of physiology, value, and pitfalls in clinical practice. Paediatric anaesthesia 2021;31(8):839-845. (In eng). DOI: 10.1111/pan.14208.
3. Chau A, Kobe J, Kalyanaraman R, Reichert C, Ansermino M. Beware the airway filter: deadspace effect in children under 2 years. Paediatric anaesthesia 2006;16(9):932-8. (In eng). DOI: 10.1111/j.1460-9592.2006.01895.x.
4. Cressoni M, Gotti M, Chiurazzi C, et al. Mechanical Power and Development of Ventilator-induced Lung Injury. Anesthesiology 2016;124(5):1100-8. (In eng). DOI: 10.1097/aln.0000000000001056.
5. King MR, Feldman JM. Optimal management of apparatus dead space in the anesthetized infant. Paediatric anaesthesia 2017;27(12):1185-1192. (In eng). DOI: 10.1111/pan.13254.