

In the November 4, 2024 PAAD: You did an Allen test, didn’t you!? Rethinking pre-procedural assessment for arterial line placement https://ronlitman.substack.com/p/you-did-an-allen-test-didnt-you-rethinking Shawn Jackson, Ethan Sanford and Justin Lockman reviewed recent studies and concluded that an Allen’s test does not enhance safety when cannulating the radial artery to establish intraarterial monitoring. Are they correct?
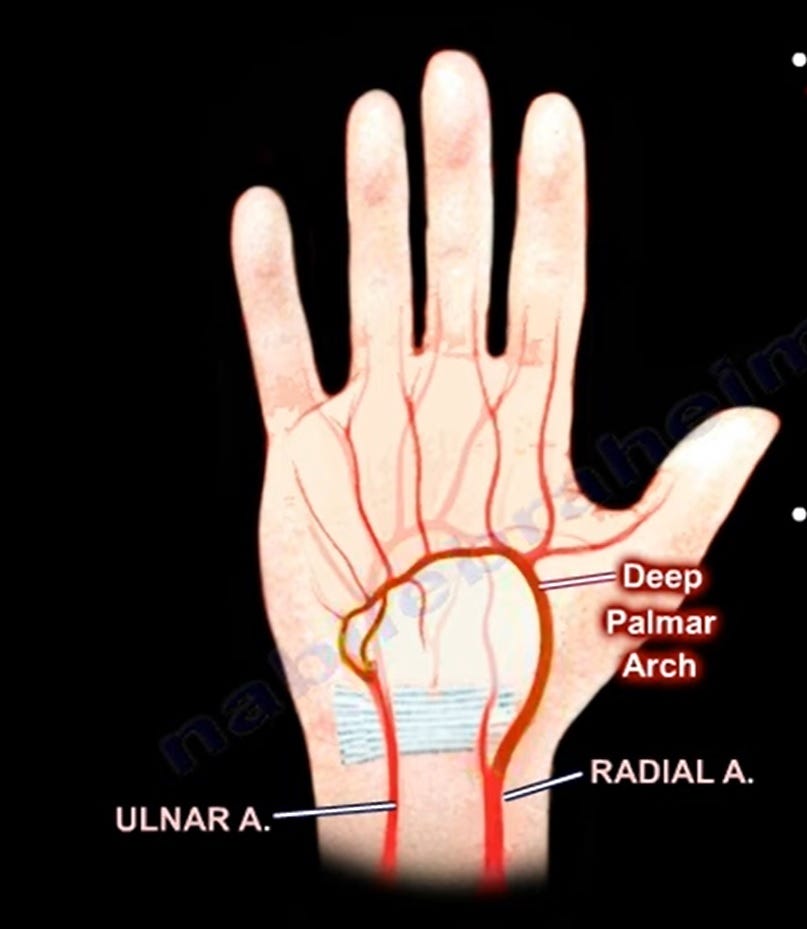
What is the Allen test and why was it used? In 1929, Edgar V Allen published, “Thromboangiitis Obliterans: Methods of Diagnosis of Chronic Occlusive Arterial Lesions Distal to the Wrist With Illustrative Cases”.1 Allen’s original intent was to diagnose the presence of obliterative vascular process in the radial and ulnar arteries. The test infers the competence of the circulation of the hand provided by the ulnar and radial arteries, via the palmar arch. Allen stated, “Accurate diagnosis is not aided by time-consuming mechanical contrivances…Critical examination by vision and palpation…are sufficient.”1 The intuitive application of Allen’s observations was that:
When bilateral occlusion of the radial and ulnar arteries produce palmar pallor
and release of the occlusion of one of the arteries of the wrist is followed by return of the other pulse and a plethoric hue to the entire hand
it can be inferred that the single unoccluded artery provides sufficient circulation to the hand
Is the inference of the presence of adequate circulation in the hand when performing the Allen’s Test valid? As pointed out by Jackson, Sanford and Lockman, the answer is no! Reviewing classic studies investigating this question is instructive confirming this conclusion.
Greenhow noted that incorrect performance of the Allen’s Test could produce a false result.2 Bedford and Wollman investigated complications of radial artery cannulation employing physical examination and Doppler flow measurements.3 Several of their patients who developed transient radial artery occlusion post cannulation displayed physical signs of inadequate circulation of the hand in spite of the presence, “…of brisk ulnar-artery flow by Allen’s test prior to cannulation.”3 Fuhrman, Pippin, Talmage and Reilley countered Allen’s assertion that “…mechanical contrivances…” weren’t necessary.3 They employed plethysmography and pulse oximetry to refine the assessment of circulation of the hand, finding plethysmography to be superior.
What might the takeaway message be from remembering the classic studies with added confirmation by current investigations? Whether using physical examination (assessment of pulse and observation of skin color) or more sophisticated monitoring techniques (plethysmography, pulse oximetry, Doppler flow measurements), the Allen’s test is a historically interesting attempt to answer a question (will radial artery cannulation result in morbidly inadequate circulation of the hand) that to this day remains unanswered.
Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Allen EV. Thromboangiitis Obliterans: Methods of Diagnosis of Chronic Occlusive Arterial Lesions Distal to the Wrist With Illustrative Cases. Am J Med Sci. 1929; 178(2): 237-243
2. Greenhow DE. Incorrect performance of Allen’s Test-Ulnar Artery Flow Erroneously Presumed Inadequate. Anesthesiology 1972; 37(3): 356-357
3. Bedford RF, Wollman H. Complications of Percutaneous Radial-artery Cannulation: An Objective Prospective Study in Man. Anesthesiology 1973; 38(3): 228-236
4. Fuhrman TM, Pippin WD, Talmage LA, Reilley TE. Evaluation of collateral circulation of the hand. J Clin Monit 1992; 8: 28-32