
Reader response
Myron Yaster MD

From Vikas O'Reilly-Shah, MD, PhD, FASA, Professor of Anesthesiology & Pain Medicine, University of Washington | Seattle Children's Hospital
One source of poorly conducted research only lightly touched upon in the PAAD are the incentives wrought by academia itself. The authors write, "[W]e absolutely understand the need to publish for purposes of academic advancement and recognition. The urge to publish in any Pubmed cited journal, and yes to bend the facts, are overwhelming."
Indeed, it is these incentives that are at the very root of the problem. I daresay that the bulk of clinicians in academic practice have very little interest in research or publishing per se, and yet promotion criteria on non-tenure line promotion tracks still require non-negligible scholarly output. These are the very faculty, because of their lack of familiarity with the nuances of (e.g) Pubmed-indexing, that will fall prey to 'Greetings of the day' emails from predatory journals, offering to publish their paper or even make them an editor of the journal! These are the very faculty that will sign onto, conduct, and publish low quality papers - not out of any sort of ill intention, but simply because this is not what they do. These are clinicians and clinician-educators, folks who enjoy taking care of patients and teaching medical students, residents, and fellows. You wouldn't expect a board-certified internist to conduct a safe anesthetic; why would you expect a board-certified anesthesiologist to conduct a high-quality graduate or PhD level research study, without the additional training it takes to acquire competence in that arena?
What I would propose, and I understand this sounds crazy and runs counter to (one, perhaps archaic, view of) the academic mission, is that promotion criteria themselves should be updated to keep up with the times and to recognize the threats posed by misaligned incentives. Here at the University of Washington, we do indeed provide credit for what we term 'scholarship of dissemination' (e.g. PBLD or clinical practice guidelines) and 'scholarship of teaching' (e.g. curriculum development, podcasts). Even still, these 'equivalents' only count towards half of the publication requirements. I haven't conducted a formal survey, but I imagine that this is still on the very liberal end of the spectrum.
For those of you who have read the YA Red Rising series, you'll recognize this quote: "A fool pulls the leaves. A brute chops the trunk. A sage digs the roots." To get at the root cause of predatory journals and poorly conducted research, we must address and align the incentives of academia with the realities of what people want to do and are capable of doing competently based on their training. Otherwise, academia has only itself to blame for this continuing threat to the evidence base in medicine.
From Lynn Martin MD MBA, Professor Emeritus, Seattle Children’s, Department of Anesthesiology and Pain Medicine, University of Washington School of Medicine
As usual, I enjoyed reading my daily dose of education (or in this case re-education) provided by the excellent editorial board at PAAD and my mentors (Drs. Yaster and Maxwell). I had previously read the comprehensive and excellent APSF review of monitoring for detection of opioid-induced respiratory depression authored by Drs. Vecchione and Monitto.1
Myron loves to take controversial positions on subjects to stimulate dialog, so please allow me to follow his lead. Opioids have a very long list of side-effects that can produce serious life-threatening complications, such as respiratory depression.2 So why do we continue to insist that “opioids are an essential building block for moderate to severe pain”? Rather than worrying about how best to monitor our patients that receive opioids, should we not be asking ourselves are these opioids truly necessary? We commonly give opioids without thinking as part of our balanced anesthetic, never asking this important question. I have become convinced that in many cases the answer is no opioids are needed because there are proven, viable alternatives for opioids both intraoperative and postoperatively, thus allowing us to completely bypass the risk of respiratory depression. Now let me backup this bold statement with data!
Previously we have published multiple manuscripts on our now common practice of opioid-free anesthesia (OFA) in Seattle.3-5 The basis for this approach is the use of multimodal analgesia and maximizing the use of regional anesthesia with ongoing monitoring of our daily outcomes so we can continuously learn and further improve. Last year we published a 5-year summary of these efforts in which 41,260 ambulatory and hospitalized patients received OFA.6 In that publication we highlight two examples in which OFA appears to not just be equivalent, but actually superior (ambulatory T&A for obstructive sleep apnea patients and inpatient non-invasive laparoscopic appendectomy). Based partly on this practice, our surgeons now treat a select subpopulation of appendectomy patients on an ambulatory basis, thereby completely avoiding hospitalization.
I have faced many very skeptical audiences and readers who frankly believed we have ‘cooked’ or ‘ignored’ data. Yet our experiences and satisfaction with this approach is real and continuously growing and improving. As of 6/26/2024, there have been 28,966 ambulatory patients who have received OFA, continuously exceeding 99% in our ambulatory surgery center since 1/1/2023.

At the hospital 33,234 patients have received OFA with a mean rate of 62% of cases since 1/1/2023.
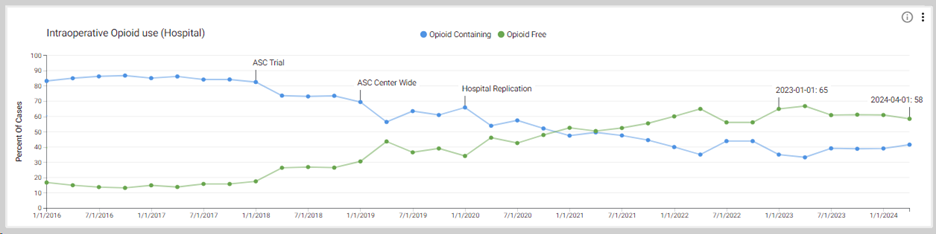
This is a cumulative total of 62,200 patients that have now received OFA at Seattle Children’s since the formal start of these efforts in 2018. Stealing the famous quote from Dr. John Colins Warren following the first public demonstration of ether on 10/16/1846, “Gentlemen, this is no humbug!”. In this modern era of anesthesia, must we routinely be giving opioids? The clear answer is NO! I challenge PAAD readers to start critically thinking about their use of opioids for each case. Are they turly necessary? If yes, can you safely lower the dose? Any efforts to reduce their use will lessen the risk of opioid-induced respiratory depression, it’s associated life-threatening complication, and even the need for monitoring.
References
1. Vecchione T, Monitto C. Opioid-Induced Respiratory Depression—Pediatric Considerations. Anesthesia Patient Safety Foundation. Anesthesia Patient Safety Foundation. 06/2024 (https://www.apsf.org/article/opioid-induced-respiratory-depression-pediatric-considerations/?utm_source=APSF+Newsletter+Email+-+External&utm_medium=email&utm_campaign=EMAIL_CAMPAIGN_2024_06_01).
2. Lavand'homme P, Steyaert A. Opioid-free anesthesia opioid side effects: tolerance and hyperalgesia. Best Pract Res Clin Anaesthesiol.2017;31:487-498. (PMID: 29739537).
3. Franz AM, Dahl JP, Huang H, et al. The development of an opioid sparing anesthesia protocol for pediatric ambulatory tonsillectomy and adenotonsillectomy surgery-A quality improvement project. Paediatr Anaesth. 2019;29(7):682-689. doi:10.1111/pan.13662. (PMID: 31077491).
Franz AM, Martin LD, Liston DE, et al. In Pursuit of an Opioid-Free Pediatric Ambulatory Surgery Center: A Quality Improvement Initiative. Anesth Analg. 2021;132(3):788-797. doi:10.1213/ANE.0000000000004774. (PMID: 32282383).
Chiem JL, Franz A, Bishop N, et al. An Opioid Sparing Anesthesia Protocol for Open Inguinal Hernia Repair: A Quality Improvement Project. Pediatr Qual Saf. 2022;7:e548; doi: 10.1097/pg9.0000000000000548 (PMID: 35369423).
Martin LD, Franz AM, Rampersad SE, et al. Outcomes for 41 260 pediatric surgical patients with opioid-free anesthesia: One center's experience. Paediatr Anaesth. 2023;33(9):699-709. doi:10.1111/pan.14705. (PMID: 37300350).
From Henry Rosenberg MD
Mildred Thornton Stahlman, Pioneer in Neonatal Care, Dies at 101
Fascinating woman-pioneer in neonatal critical care that most of us have never heard .of