

My apologies: Dr. Feldman’s response was not posted in its entirety. I am reposting the correct version
From Richard Blum MD, Boston Children’s Hospital on priming the circuit
I thought this was an important topic in terms of the need to increase the circuit concentration quickly in patients that are uncooperative which unfortunately is sometimes the case despite attempts at non-medication based preparation techniques as well as after inadequate effectiveness of pre medication. The one technique that I did not see addressed was “ventilatory assisted priming” (VIP) which is a term I do not use but involves using relatively low flow rates e.g. 4 L/min, occluding the circuit and pumping the anesthesia bag. I believe this opens and closes the inspiratory and expiratory limbs of the circuit and can lead to very high concentrations quickly and with less anesthetic gas waste. I sent an email to Diane Gordon who has written on this to get her thoughts but would be interested in others thoughts on the effectiveness of this technique to rapidly increase the inspiration concentration of inhalation agent and decreasing waste gas and cost and less impact on the environment.
In response Jeffrey Feldman MD
Diane and I have been writing about priming recently in the PAAD in response to questions. Our paper on environmentally responsible mask induction explores priming in some detail (Gordon, D. & Feldman, J. Environmentally Responsible Mask Induction. Best Pr. Res. Clin. Anaesthesiol. 38, 321–331 (2024). Clearly, priming can play a useful role to shorten the time required to reach an effective inspired concentration of Sevoflurane during mask induction. We advocate for a process of emptying the reservoir bag once while starting fresh gas flow at a rate that approximates the patient’s minute ventilation. The rationale for this approach is to limit FGF to the maximum needed to eliminate rebreathing in the circle system while minimizing the amount of time FGF is set to a high level. I have used this approach repeatedly for numerous patients using Draeger Apollo and Perseus workstations and achieved satisfactory mask inductions. Admittedly, I have not collected data demonstrating the rate of change of anesthetic concentration. Other methods of priming are discussed in the paper although not specifically what you call Ventilator Assisted Priming. It is clear based upon machine design that if the end of the breathing circuit is occluded, when squeezing the reservoir bag the same pressure to open the inspiratory valve will be exerted on the expiratory valve to keep it closed. As a result, squeezing the reservoir bag while the circuit is occluded will not prime the portion of the circuit on the patient side of the inspiratory and expiratory valves. Thanks for raising this question as it provides an opportunity for some further clarification. It will take us into the weeds a bit on anesthesia machine design.
I found one published study specifically on the topic of Ventilator Assisted Priming. (Ali MS, Aamir R. Ventilator-assisted priming of an anaesthesia circuit (VAP technique): An exploratory study. Indian J Anaesth 2022;66:763-8. ) In that study, they showed that Ventilator Assisted Priming with an occluded circuit resulted in a significantly faster rise in inspired Sevoflurane concentration to 6% than just passive FGF even after emptying the reservoir bag. To understand why they observed this result, it is very important to recognize both how they did the ventilator assisted priming (VAP) and the type of anesthesia machine used.
VAP was performed with the circuit occluded and the mechanical ventilator set in volume mode. While they used different settings for tidal volume, they indicate that the actual tidal volume delivered did not change much despite different settings. This is not at all surprising and was due to the fact that the circuit was occluded and the ventilator simply stopped delivering volume when the pressure limit of 40 cmH2O was reached. The did not test a process of pumping the reservoir bag to simulate mechanical ventilation. Why did they observe such a significant reduction in time to a sevo concentration of 6%? The answer lies in the design of the anesthesia machine they used.
The Drager Fabius machine uses a piston ventilator and a somewhat unique circle system design. The same design is used in all Draeger piston ventilator machines – Primus/Apollo and Atlan. The unique aspect of this circle system is the addition of a FGF decoupling valve which sits between the fresh gas inflow and the ventilator. The following is a circuit diagram for the piston ventilator based machines.
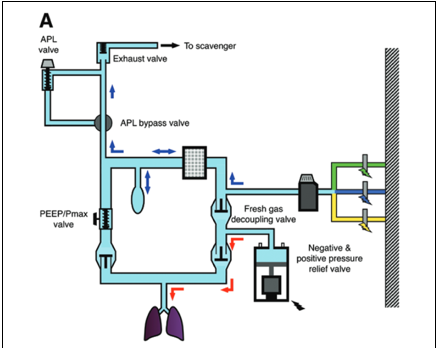
Article Reference for this figure: Hendrickx, J. F. A. & Wolf, A. M. D. The Anesthesia Workstation. Anesthesia Analgesia 127, 671–675 (2018). Reproduced courtesy of Andre Dewolf.
The important point to observe here is that when the ventilator is attempting to deliver tidal volume it will hold the decoupling valve closed and open the inspiratory valve pushing some gas into the circuit. During exhalation, the piston retracts opening the decoupling valve and drawing some fresh gas in to the circuit. With the circuit occluded, the tidal volume actually delivered will be based upon the compliance of the breathing circuit and the pressure achieved (40 cmH2O) in their study.
What can we conclude about ventilator assisted priming? When using a machine with a piston ventilator and fresh gas decoupling valve, actually using the mechanical ventilator to prime the circuit can shorten the time needed to reach an inspired Sevoflurane concentration of 6%. The same result would not be expected in machines with more traditional circle systems where there is no decoupling valve and the ventilator is in the same position in the circuit as the reservoir bag. VAP as studied and reported by Ali and Amir is not the same as squeezing the reservoir bag which would not be expected to be different between anesthesia machine designs. In all the designs, the pressure resulting from squeezing the reservoir bag will exert equal forces to open the inspiratory valve and hold the expiratory valve closed.
I hope this is helpful and not too far into the weeds. There is opportunity for studies to demonstrate the results that can be obtained by different approaches to priming. There will be differences between anesthesia machines. Careful scrutiny of the various circuit designs can lead to an understanding of the results that can be expected with different priming techinques. It is also easy to try different approaches and observe the rate of rise of anesthetic concentration during mask induction as well as most importantly, the success of the mask induction process. It is not as easy to document the anesthetic agent consumption that results from the priming process and there is the potential for significant waste. The rationale for the process described by Diane Gordon and I in our article is to find the balance between a rapid rise of anesthetic concentration to achieve a successful mask induction without generating excessive waste.
Appreciate the thoughtful question.