
Reader response
Myron Yaster MD

From Suryakumar Narayanasamy, MBBS, MD
Neuner et al. published a follow-up letter in the May 2026 issue of Anesthesia & Analgesia responding to Pai et al. Their main critique is that the study’s conclusions rely on ROC analysis with very low specificity, limiting clinical usefulness—a concern I also raised during our PAAD review.
Selection bias is another key limitation given the small number of GLP-1 users included. Additionally, inter-observer variability was not independently assessed. Although gastric ultrasound is known for good inter-observer agreement, this should be validated to ensure consistency. In practice, interpretation can vary. I have seen cases labeled “high risk” by others that I would consider low risk due to minimal echogenic speckling in a small stomach—findings that can occur even after prolonged NPO and are not equivalent to significant solid content.
The lack of validation of the Perlas formula in this population is less concerning, as it remains the most widely used tool despite its limitations and mainly applies to clear liquids, not solids. However, the study does not specify how many high-risk patients had liquids versus solids, making it difficult to assess the formula’s impact on the results
References:
1. Neuner, Matthias MD; Poeran, Jashvant MD, PhD; Tailor, Maya BS; Memtsoudis, Stavros MD, PhD, MBA; Cozowicz, Crispiana MD; Panzer, Oliver MD. Assessment of Gastric Content Using Gastric Ultrasound in Patients on Glucagon-Like Peptide-1 Receptor Agonists: Selection Matters. Anesthesia & Analgesia 142(5):p e81-e83, May 2026. | DOI: 10.1213/ANE.0000000000007988
2. Pai SL, Nimma SR, Beam WB, et al. Assessment of Gastric Content Using Gastric Ultrasound in Patients on Glucagon-Like Peptide-1 Receptor Agonists Before Anesthesia. Anesthesia and analgesia 2026;142(4):640–649. (In eng). DOI: 10.1213/ane.0000000000007764
From Mark Schreiner MD
Whether or not delayed gastric emptying due to GLP-1 receptor antagonists results in GFVs outside the normal range and actually create an increase in risk is yet to be determined. If there is an increased incidence of aspiration, is it due to the drug, the patient’s diabetes or obesity (difficult airway) or other factor. And even if gastric emptying is delayed, does that in itself matter?
28 years ago, I advocated that we stop using gastric fluid volume (GFV) of > 0.4 mL/kg as a surrogate marker for patients being at high risk of pulmonary aspiration. (1) GFV has absolutely no proven association, independent of other risk factors, for aspiration. In my editorial, I concluded by saying “It is time to put an end to using the criteria of Roberts and Shirley (2), a surrogate measure with no proven clinical basis, and to put an end to discussions of risk based on studies whose designs fail to meet basic criteria for adequate evidence. The discussion should be shifted from a focus on the GFV at the time of induction of anesthesia to the patient’s characteristics and comorbid conditions, as well as to the anesthetic practices that place patients at risk of pulmonary aspiration of gastric and intestinal contents.”
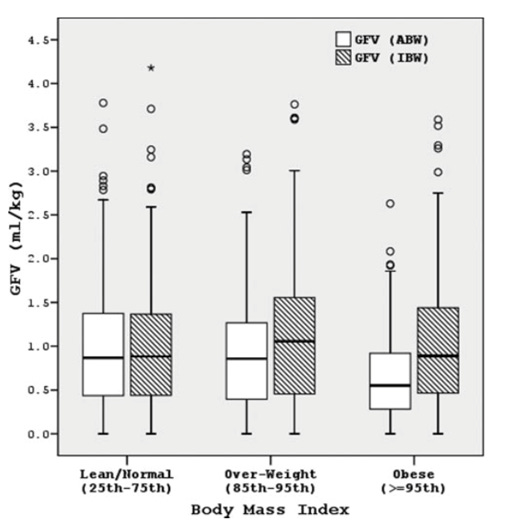
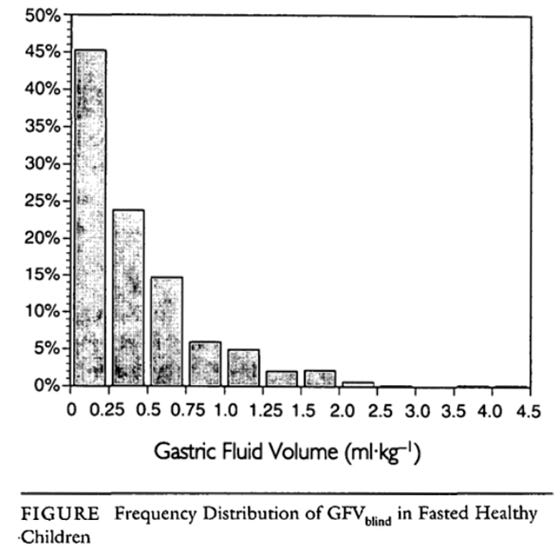
It turns out that normal children having elective surgery commonly have large GFVs with 5% have a GFV between 1.5 - 4.5 mL/kg. (Figures below from (2) and (3)).
Pulmonary aspiration of gastric contents is fortunately a rare event in pediatric anesthesia practice, with an incidence on the order of 1:3000 – 1:10,000 anesthetics.(4 – 7) The EUROFAST study, published in 2025, included over 300,000 anesthetized children and compared 3 fasting protocols. The incidence of aspiration ranged from 0.96 – 1.83:10,000. (7) None of the 420 who aspirated, died but 134 required some escalation in care.
Since so many children present with “large” GFVs, if GFV by itself were actually a risk factor for pulmonary aspiration, it should be more evident. So let’s all agree to stop referring to children with GFVs within normal ranges as being at risk for pulmonary aspiration. Do GLP-1 receptor antagonists increase GFV beyond the normal range? I don’t know. Instead, let’s focus our attention on actual risk factors for pulmonary aspiration such as emergencies, bowel obstruction, difficult airway, incompetent esophageal sphincter, etc. Let’s do some research and document the GFV and incidence of aspiration in children taking GLP-1 inhibitors to find out if there is an actual clinical problem.
Just a suggestion: until GFV is proven to be a useful surrogate, perhaps a little less time, money and effort should be spent on ultrasound measurement of GFV.
References
1. Schreiner MS. Gastric fluid volume: is it really a risk factor for pulmonary aspiration? Anesth Analg. 1998;87(4):754-6.
2. Cook-Sather SD, Gallagher PR, Kruge LE, … Litman RS, Schreiner MS. Overweight/obesity and gastric fluid characteristics in pediatric day surgery: implications for fasting guidelines and pulmonary aspiration risk. Anesth Analg. 2009; 109(3):727-36.
3. Cook-Sather SD, Liacouras CA, Previte JP, Markakis DA, Schreiner MS. Gastric fluid measurement by blind aspiration in paediatric patients: a gastroscopic evaluation. Can J Anaesth. 1997;44(2):168-72.
4. Warner MA, Warner ME, Warner DO, Warner LO, Warner EJ. Perioperative pulmonary aspiration in infants and children. Anesthesiology. 1999 Jan;90(1):66-71.
5. Kelly CJ, Walker RW. Perioperative pulmonary aspiration is infrequent and low risk in pediatric anesthetic practice. Paediatr Anaesth. 2015;25(1):36-43.
6. Andersson H, Zarén B, Frykholm P. Low incidence of pulmonary aspiration in children allowed intake of clear fluids until called to the operating suite. Paediatr Anaesth. 2015; 25(8):770-777.
7. Frykholm P, Modiri AR, Klaucane A, Beck CE, Bouvet L, Isserman RS, Oshan V, Stricker PA, Quintão VC, Frithiof R; EUROFAST Collaborative Group. Impact of liberal preoperative clear fluid fasting regimens on the risk of pulmonary aspiration in children (EUROFAST): an international prospective cohort study. Br J Anaesth. 2025;135(1):141-147.
From Richard Newton MBBS FRCA, Consultant Paediatric Anaesthetist, UNIVERSITY HOSPITALS SUSSEX NHS FOUNDATION TRUST)
I read with interest the articles here and here this week, including the editorial. I think we have to be very careful following this guidance based on the potential risk of aspiration.
Aspiration, rightly, is at the forefront of every anaesthetists mind when giving an anaesthetic and anything to reduce this risk should be undertaken. However, to date, there has been no study which showed that increased gastric volume increases your chance of gastric aspiration.
Whilst we use 1.5mL/kg on gastric ultrasound as a cut off, even in health there are many patients with over this volume. Elkin in his metanalysis in 2025 (anaesthesia) showed an increase in gastric volume with GLP1 but no increase in gastric aspiration with over 185,000 patients.
As you are aware the literature is muddy due to many heterogenous studies. The time you have been on a GLP1 appears to be important. If you have not had an increase in dose and been on it for over 12 weeks it appears that your gastric emptying rates return to normal. Whereas if you stop a dose or even at subtherapeutic dose, as you come off / decrease the drug, we once again have delayed gastric emptying.
By stopping GLP1 in cardiac or diabetic patients we may be doing more harm and all due to the perceived risk of aspiration.
Moving forward, gastric ultrasound may help the individual realise that the patient in front of them has a “full stomach” and therefore this information can be used to help the individual make an appropriate airway plan. However, stopping, reducing the dose, delaying food intake does not suddenly make it “ safe” to give them an anaesthetic. We are airway experts and this is just another group who needs careful planning with airway expertise to reduce the chance of aspiration.
Just my two pence piece worth. I think we are missing the wood from the trees. I wonder if we will be doing more harm than good.
From Jonathan D Blank MD
I have been a long time proponent of decreasing oxygen percentage on induction As a peds anesthesiologist I have trained with the Nitrous Oxide and Oxygen set at 5-6/3-4 liters. As children are at higher risk desaturation I have noted that in most “healthy “ children - not neonates and not septicemia patients - keeping O2 at 40-60% is more than adequate. In neonates I strive for 25-30% for risk of ROP and have been able with proper ventilator maintain 21-22%. I have seen the lack of decreased O2 concentrations in adults but now with many CRNAs who come from a world of titrating oxygen. There is better results. The concept of atelectasis is easy way to discuss as long term cardiac, kidney or lung damage is harder to put a finger on. Hopefully the next cohort of anesthesiologists can be trained correctly with more information and resources like these articles
From Sorin J. Brull, MD, FCARCSI (Hon) APSF Newsletter Editorial Board responding to respiratory monitoring in the newly born here
The ExSpiron respiratory volume monitor (Senzime AB, Uppsala, Sweden) is a noninvasive, bioimpedance-based system designed for continuous quantitative assessment of ventilation in spontaneously breathing and mechanically ventilated patients, including neonates, infants, and children. Using disposable thoracic electrode sensors, the device measures changes in electrical impedance during respiration to calculate tidal volume, respiratory rate, and minute ventilation in real time. Unlike pulse oximetry and capnography, which may detect respiratory compromise late and do not directly measure ventilation, ExSpiron provides continuous objective assessment of respiratory status, particularly valuable in pediatric patients with low tidal volumes and rapid respiratory rates. Clinical studies have demonstrated good agreement between ExSpiron measurements and spirometry in neonatal and pediatric populations. The technology has been applied in operating rooms, intensive care units, post-anesthsia care units, and procedural sedation settings, where it may facilitate earlier recognition of hypoventilation, apnea, and respiratory deterioration, thereby improing perioperative and critical care respiratory monitoring and patient safety
References
1. Atkinson DB, Sens BA, Bernier RS, Gomez-Morad AD, Imsirovic J, Nasr VG. The Evaluation of a Noninvasive Respiratory Volume Monitor in Mechanically Ventilated Neonates and Infants. Anesth Analg. 2022 Jan 1;134(1):141-148. doi: 10.1213/ANE.0000000000005562. PMID: 33929346.
2. Gomez-Morad AD, Cravero JP, Harvey BC, Bernier R, Halpin E, Walsh B, Nasr VG. The Evaluation of a Noninvasive Respiratory Volume Monitor in Pediatric Patients Undergoing General Anesthesia. Anesth Analg. 2017 Dec;125(6):1913-1919. doi: 10.1213/ANE.0000000000002029. PMID: 28759491.