
Reader response
Myron Yaster MD

From Stephen Gleich, M.D., FAAP, Mayo Clinic on intraoperative handoff checklist
Thank you for your excellent review and summary of “Checklist for intraoperative handoffs: does less improv improve harmony?.” As a former coporate jet pilot, I have a deep and strong appreciation of standardized processes, including the use of structured briefings and checklists. While these standardized handoff checklists are helpful and almost certainly improve care, we need to assure the checklist design maximizes human performance.
As an example, take a look at the intraoperative handoff tool that is posted on the SPA website (https://pedsanesthesia.org/wp-content/uploads/2018/08/Intraoperative-Handoff-Tool-FINAL-Nov-2012.pdf). Imagine receiving this structured handoff from a colleague – my mind would definitely wander prior to completion of the handoff. While extremely comprehensive, there is a lot of “routine” information that is conveyed early in the checklist.
Studies on human performance show us that information presented first in a handoff or briefing is better retained. Thus, we should be relaying the most important information as early as possible in the handoff.
Utilizing this “law of primacy,” a major airline recently revised the way the flight crew performed their briefings. They found that:
“Our briefings, like so many in the aviation industry…had become so overloaded and were so often conducted by rote that many crews were either choosing not to adhere to the seemingly irrelevant policy or they dutifully followed it, only to find out later, that what they spent so much time briefing wasn’t focused on or directed toward what they should have been briefing.”
Consequently, the airline changed to a “Threats-Plan-Considerations” briefing structure. With this model, threats are first identified in the briefing. Such threats are very broad and can be anything from adverse weather, to delays, crew fatigue, environmental considerations, production pressure, to an unruly passenger, etc. Following Threat identification, the Plan and Considerations portion of the briefing discuss how to manage the threats identified.
Now imagine receiving a handoff from a colleague on a routine case that first addressed the threats. Specifically, what is different or unique about this otherwise routine case that I need to know about? With this approach, additional errors may be prevented.
Saha AK and colleagues should be complimented for their inclusion of “Key Events” and “Situational Awareness” sections in their electronic handoff checklist. However, they might consider moving those sections up to an earlier part of the handoff for maximal retention.
Thank you again for the excellent review. I strongly advocate for using checklists and standardized processes as much as possible – with the most critical information conveyed first.
From Leonardo Gendzel MD, Levine Children’s Hospital, Charlotte NC on look a like drugs
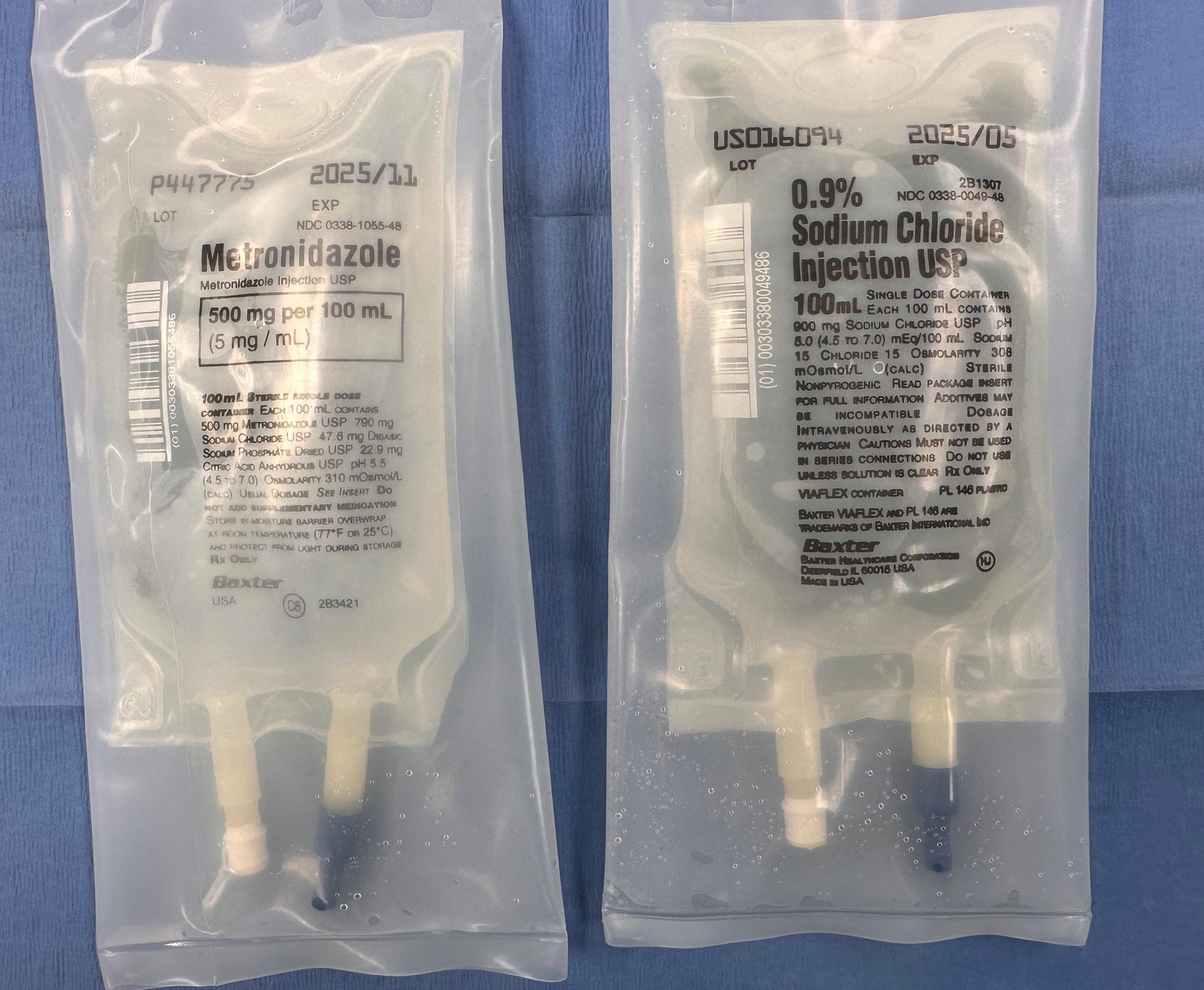
The timing of today’s PAAD was incredible. I am on call today and was preparing a 100mL bag for a 2 week old lap pyloric and look what I found in the same bin! Good that I checked! I showed it to the CRNA I was working with and she said she's been finding similar look a like bags and vials in wrong bins as well!!
From Andrew Giustini, MD, PhD, Assistant Professor, Pediatric Cardiac Anesthesiology, Department of Anesthesiology and Perioperative Medicine, Oregon Health and Science University on look a like drug vials
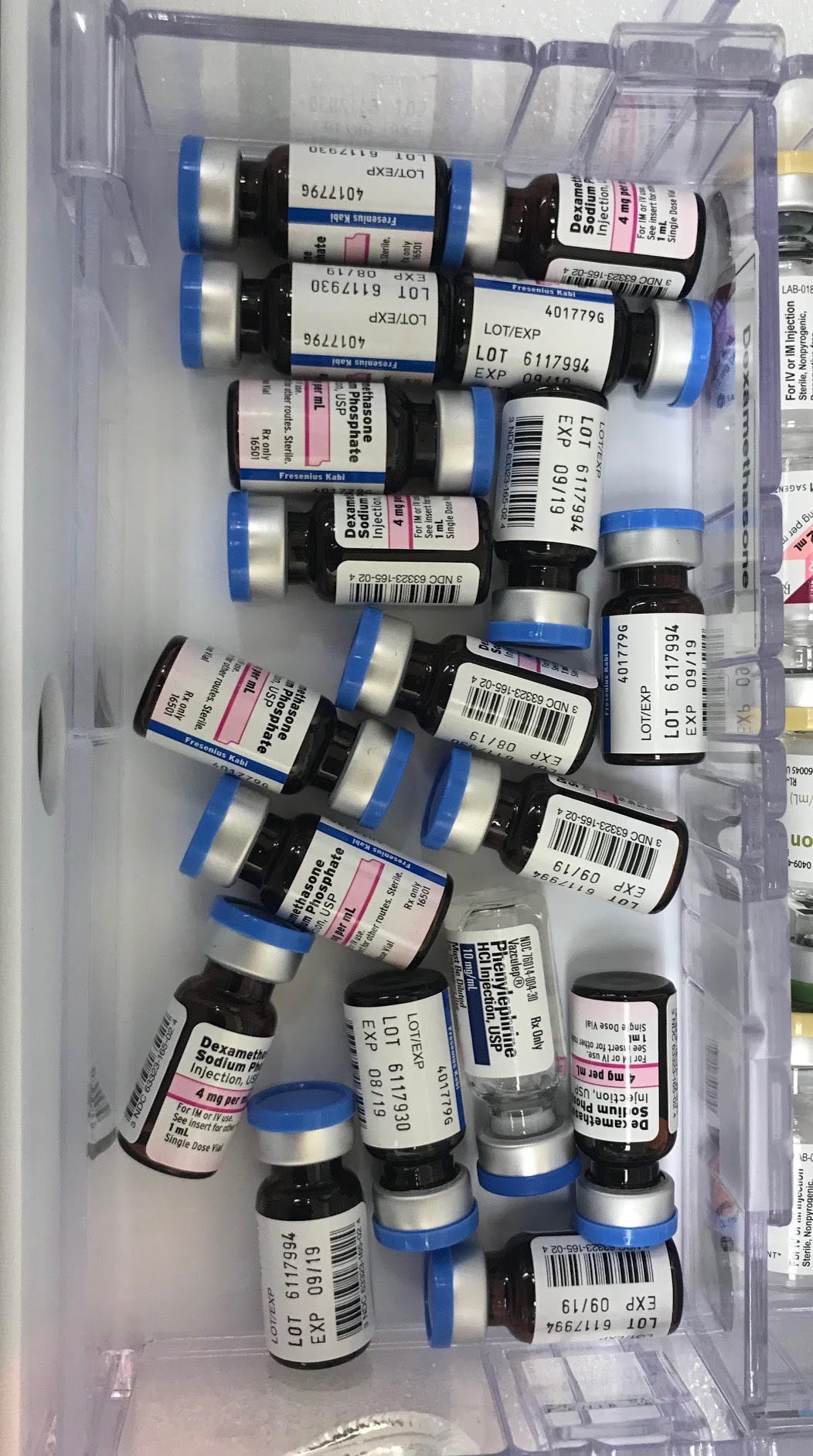
I completely agree with the idea that we need standardization of bottle shapes and lid colors to visually separate classes of drugs to reduce the risk of medication errors. This is a picture I like to share with trainees that I took of an OR drug drawer when I was a resident. See if you can spot the potentially fatal vial camouflaged amongst the safer vials. I use this to emphasize why they must always read the labels of what they are giving.
From Lynn D. Martin, MD MBA, Professor Emeritus, Anesthesiology and Pain Medicine, University of Washington School of Medicine on look a like drugs
I read with interest your review of the manuscript by Bitan, O’Connor, and Nunnally last week. (1) I applaud these authors efforts to study the most serious gap in the safety of the modern practice of anesthesiology. I also thank the editors of the PAAD for selecting this manuscript and their thought-provoking commentary. I was faced with this very issue while serving as Anesthesiology Chief at Seattle Children’s. The hospital experienced two separate medication errors that led to serious safety events within a 6-month period (fortunately not in the operating rooms). Hospital leaders paused elective clinical care for a day to hold an all-hands Safety Summit. Every departmental leader was instructed to conduct and improve medication safety in their practice. I would like to share several of our findings.
With support from the OR pharmacy and hospital continuous improvement teams, the anesthesiology department recognized the unique medication processes practiced by anesthesiologists with the bypassing of several safety checks routinely used elsewhere throughout the hospital. Therefore, using Institute for Safe Medication Practices (ISMP) guidelines and reviewing the literature, we conducted a formal failure mode effects analysis. (2) Rather than wait for external industry changes (all of which would be very useful), we focused on measures to reduce our risks. Five changed were implemented over a 12-month period: (1) reorganization of anesthesia medication storage, (3) testing a standardized anesthesia work cart medication template, standardized syringe labeling, (4) 2-provider infusion check, and (5) create a departmental medication practice guideline. Compliance with these new practices increased, resulting in a reduction in median medication error rate from 1.56 to 0.95 per 1000 anesthetics. The medication cart top template is an excellent example of a forcing function to help standardize provider practice (in this case medication setup on the work cart). (3) In simulated emergencies odds of medication dosing errors reduced using the template (OR 0.21, 95% CI 0.07 – 0.66). These results may be due to reduced cognitive load in an emergency. Medication errors reaching the patient decreased from 1.24/1000 anesthetics (0.85-1/79) to 0.65/1000 anesthetics (0.39-1.09).
In closing, I absolutely agree with the editors that anesthesiologists in general and anesthesia societies in particular (APSF, SPA, ASA, etc.) need to band together to implore change within the pharmaceutical industry to implement simple changes and standards that could enhance medication safety. Furthermore, I remind all anesthesiologists and leaders that there are numerous , simple, cost-effective interventions that can be easily implemented to reduce variation and risk for medication errors. Act now to do your part to reduce medication error risk!
1. Bitan Y, O’Connor MF, Nunnally ME. The vial can help: Standardizing vial design to reduce the risk of medication errors. Int Anesthesiol Clin. 2024 Apr 1;62(2):58-61. Doi: 10.1097/AIA.0000000000000431. Epub 2024 Jan 22. PMID: 38251720.
2. Martin LD, Grigg ED, Verma S, Latham G, Rampersad SE, Martin LD: Decreased Medication Errors in Pediatric Anesthesia Practice: Outcomes from a Failure Mode and Effects Analysis. Pediatr Anesth 2017; 27: 571-80. (PMID: 28370645)
3. Grigg E, Martin LD, Ross FJ, Roesler A, Rampersad SE, Haberkern CM, Low DKW, Carlin K, Martin LD: Assessing the Impact of the Anesthesia Medication Template on Medication Errors During Anesthesia: A Prospective Study. Anesth Analg 2017; 124:1617-25. (PMID: 280079581)
From Jennie Hamrick MD, Riley Children’s Hospital San Diego
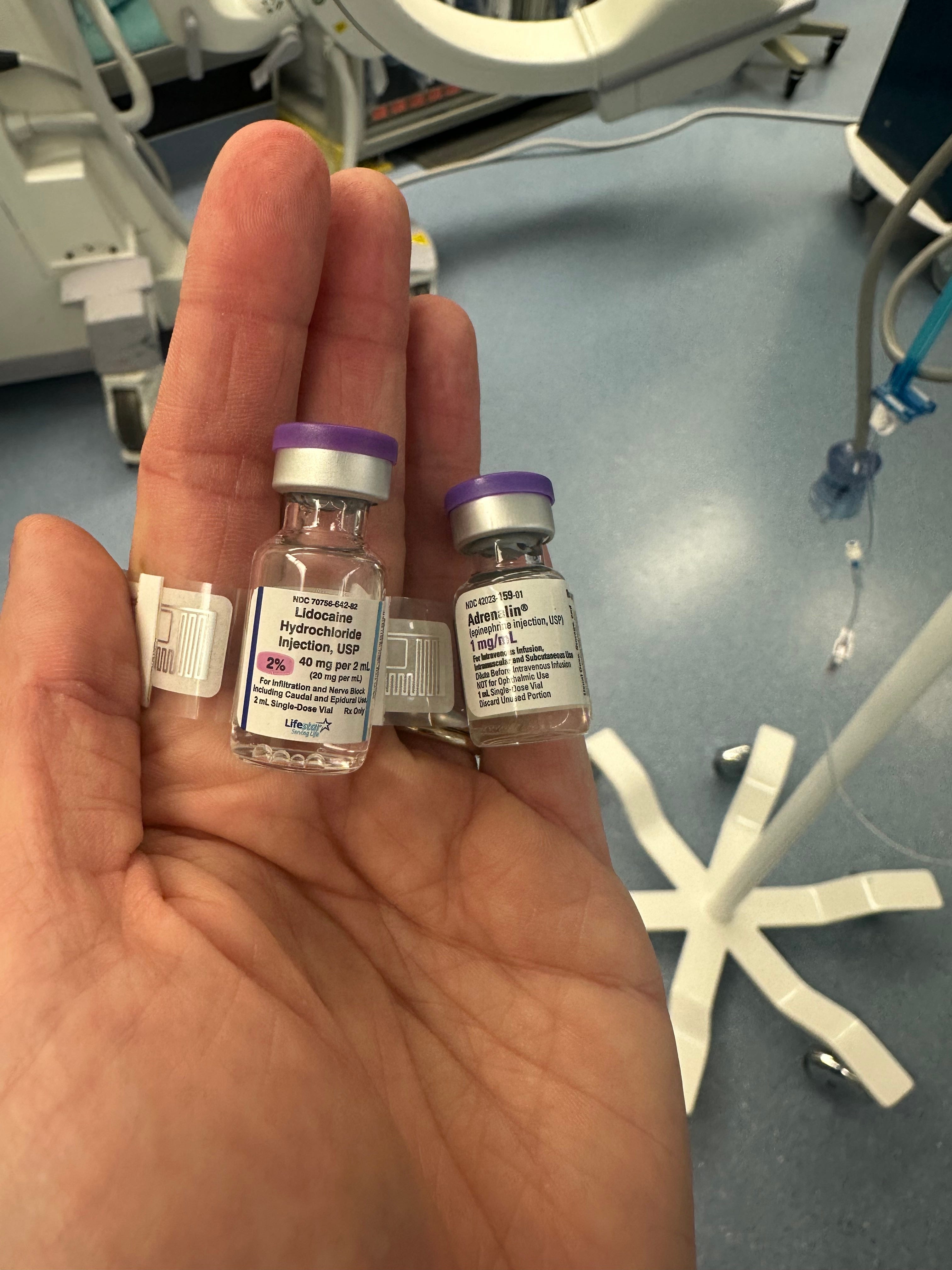
The look alike drug PAAD was timely - this lidocaine vial turned up in our drawers a week or two ago, nestled right next to the 1 mg/ml epi. Talk about potentially fatal. After I sent a photo to the pharmacy, the vials were marked with “look alike drug” stickers until they could remove the lidocaine and replace it with vials from another supplier. Yikes!
From Dan Hyman MD Chief Safety and Quality Officer, Children’s Hospital of Philadelphia
I think you misattributed the "every system" quote. It's origin is often misstated. Dr Paul Batalden from Dartmouth is the originator of the quote and not Don Berwick. Don Berwick and I and really all of us who say it all the time are being disciples of Batalden
From Walter I. Weiss MD D.ABA FASA, Chief, Pediatric Anesthesiology, NYU Langone Hospital-Long Island on look a likes
While not a definitive solution in my training decades ago we were taught to use the different size syringes (20, 10, 5, 3, and 1 cc) in combinations with different colored needles (pink, green, grey, blue, orange).
For example all paralytics were in 5 cc syringes with green needles, induction drugs in 20 cc with pink needles, etc.
I try to teach this to med students and residents. I tell them if all the labels fell off my syringes by their size and color I can tell you what’s in them.
As I age, these additional cues help prevent errors.
Just a thought.
From Justin B. Long, MD, MHI, FAAP, Associate Professor of Anesthesiology, Emory University School of Medicine, Director of Pediatric Cardiac Anesthesiology, Medical Director, Periprocedural Informatics and Medical Technology
Children's Healthcare of Atlanta at EglestonObviously, vial types/look-alike aren’t a new issue. I think watching the 60 minutes special on the Quaid twins from 2014 is mandatory watching for important historical context in medication safety for anesthesiologists: