

From anonymous on Ron Litman’s Legacy
As I listened to the PAAD Podcast about Dr Litman I remembered Ron as a colleague I had the privilege of working with in clinical and educational settings. Drs Ambardekar and Yaster have captured the essence of Ron’s gift.
Ron was curious about everything! He sought answers and made sure his students and colleagues learned too. Ron was supportive of his students (medical students, residents and fellows) always acknowledging their knowledge and skills. Ron was passionate about his own education and the same for others. Listen to the podcast to hear the sincere upbeat characterization of Ron Litman.
PAAD memorializes Ron’s passion for answers and sharing team with everyone. The anesthesiology community, worldwide, has and continues to benefit from Ron’s dedication to the best anesthesia patient care and education through PAAD. Thank you Dr Yaster for keeping Ron’s passion alive and well!
From Marc Mecoli, MD and Surya Narayanasamy, MD
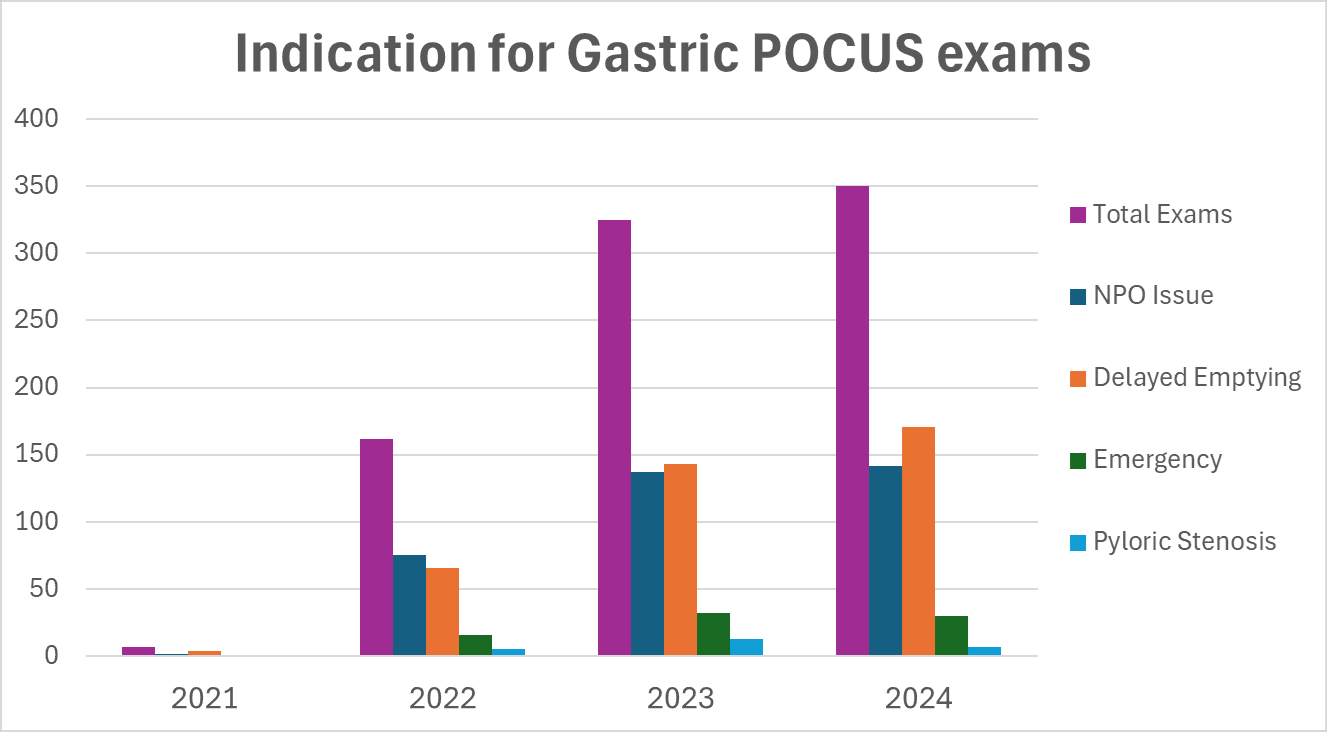
At Cincinnati Children’s we have found gastric ultrasound particularly useful and have allocated departmental resources to this specific POCUS application. By concentrating on a single modality, we have streamlined training and enhanced utilization. We increasingly use gastric ultrasound to evaluate stomach contents and guide anesthetic management in patients with NPO violation, patients with risk factors for delayed gastric emptying (including patients taking GLP-1 agonists), patients undergoing emergency surgery, and in babies with pyloric stenosis (see graphic below).
Over the last few years, we have developed a training/privileging pathway specifically for gastric ultrasound that includes didactic education, ultrasound scanning on live pediatric models, and one-on-one proctoring with expert users. We utilize the I-AIM framework described in the American Society of Regional Anesthesia and Pain Medicine expert panel recommendations on point of care ultrasound education (1). Our privileging pathway includes minimum requirements of gastric ultrasound specific CME and completion of 50 gastric ultrasound examinations (of which at least 30 are performed and interpreted by the learner). We document a procedure note describing findings in the EMR and save images and videos of all examinations for quality review. We assign a POCUS resource person to the operating room who is called to perform gastric ultrasound scans when needed.
Recently, we have enhanced our training program by aligning the clinical schedule of a POCUS mentor/trainer with a non-clinical assignment for the learner. This has significantly increased the number of proctored scans per session and accelerated the number of faculty meeting training requirements. To date, 17 anesthesiologists (roughly 20% of our faculty) have completed the training pathway. Lastly, we have integrated POCUS into our pediatric anesthesia fellowship curriculum and encourage the use of elective time to get hands-on experience in the operating room with POCUS faculty.
We envision our specialty taking a proactive role in advancing education, training, and establishing standards for gastric ultrasound and other POCUS modalities in pediatric patients. Sub-societies within anesthesia, such as ASRA, have made remarkable strides in POCUS, highlighting the impact a specialty can achieve. We may find that focusing on a specific POCUS modality is more impactful than implementing a broad spectrum of ultrasound applications for our patients. Either way, we encourage collaboration within our specialty to ensure the effective and consistent integration of POCUS into patient care.
From Vidya Chidambaran, MD, MS, MMM, FASA, FAAP Edward E. Lowe, MD Chair for Clinical and Translational Research in Anesthesia, Professor of Anesthesia, Vice Chief for Pain, Equity and Innovation, Interim Director of Perioperative pain, Division of Pain Management, Department of Anesthesia, Cincinnati Children's Hospitalon Nuss procedure analgesia
I wanted to highlight an alternative analgesia technique not mentioned in the PAAD. At Cincinnati Children's, we have implemented multimodal ambulatory erector spinae catheter (ESP) protocols for over 400 patients undergoing Nuss procedures since 2020. Patients are discharged on postoperative day 2 with the catheters, which are later removed at home by caregivers on day 5. Some patients have even traveled long distances home on postoperative days 2–3 with the catheters in place. We transitioned to ESP protocols in 2020, moving away from epidurals due to challenging transitions from epidurals to oral medications and skepticism surrounding cryoablation, which at the time lacked robust safety data and direct comparison studies1. Our team has reported our experience2, 3. Key findings from Walter et al. highlight that ESP protocols led to a shorter LOS (median 2 days vs. 3 days for epidural (EPI), p < 0.01), lower total in-hospital opioid use (median 0.57 vs. 0.82 MEq/kg, p < 0.01), and reduced post-discharge opioid duration (median 6 vs. 9 days, p < 0.01). After adjusting for covariates, ESP remained associated with shorter LOS (difference -1.2 days, 95% CI: -1.38, -1.01, p < 0.01) and decreased odds of opioid use beyond POD7 (OR 0.11, 95% CI: 0.05, 0.24, p < 0.01). Both protocols had similar emergency department visits and readmissions. ESP group did have higher rates of catheter malfunction (23% vs. 0%, p < 0.01), while the EPI group experienced more emesis (29% vs. 4%, p < 0.01).
Erector spinae plane (ESP) blocks have shown promising results, reducing opioid consumption and hospital length of stay compared to thoracic epidural analgesia in other studies as well4, 5 . Intercostal nerve cryoablation (INC) has also demonstrated benefits including shorter hospital stays and decreased intravenous narcotic use, compared to epidurals (Keller et al., 2016; Harbaugh et al., 2018). However, INC was associated with higher hospitalization costs (Perez Holguin et al., 2022), need for double lumen tube placements during GA and longer OR times (at least at our institution). A combined approach using ESP blocks with INC showed reduced opioid consumption and hospital stay compared to INC alone (Aranda-Valderrama et al., 2023). There were also reports of higher bar dislodgement rates in some studies.
In summary, erector spinae (ES) catheters are a) low-skill blocks that are easy to place with e-catheters, b) facilitate smoother transitions to oral analgesia, and c) provide longer-lasting pain relief since patients can go home with the catheters, d) offer a better safety profile compared to epidurals and potentially cryoablation, with temporary effects rather than the nerve-freezing impact of cryoanalgesia.
While INC is gaining popularity, the optimal pain management strategy for these patients remains uncertain. I remain cautiously optimistic as we await longitudinal RCTs and larger prospective studies to evaluate the incidence of neuropathic and chronic postsurgical pain associated with INC versus other techniques, that we will have a winner soon. Finally, if cryoablation proves to be a superior alternative, perhaps ultrasound-guided percutaneous cryoablation performed by trained anesthesiologists could be a viable option in the future?
References:
[1] Chidambaran V, Garcia VF, Brown RL. Are We Ready for Cryoablation in Children Undergoing Nuss Procedures? Anesth Analg. 2022;134:881-4.
[2] Abbasian N, Clay SJ, Batra M, Walter CM, Olbrecht VA, Mecoli M, et al. Multimodal continuous ambulatory erector spinae catheter pain protocol for early recovery following Nuss procedure: a retrospective cohort study. Reg Anesth Pain Med. 2022;47:421-3.
[3] Walter CM, Lee CS, Moore DL, Abbasian N, Clay SJ, Mecoli MD, et al. Retrospective study comparing outcomes of multimodal epidural and erector spinae catheter pain protocols after pectus surgery. Journal of pediatric surgery. 2023;58:397-404.
[4] Santana L, Driggers J, Carvalho NF. Pain management for the Nuss procedure: comparison between erector spinae plane block, thoracic epidural, and control. World J Pediatr Surg. 2022;5:e000418.
[5] Bliss DP, Jr., Strandness TB, Derderian SC, Kaizer AM, Partrick DA. Ultrasound-guided erector spinae plane block versus thoracic epidural analgesia: Postoperative pain management after Nuss repair for pectus excavatum. Journal of pediatric surgery. 2022;57:207-12.
From Drs. Diego Guardabassi and Javier Moriconi attendings in Paediatric Anaesthesia at Ricardo Gutierrez Children's Hospital in Buenos Aires.
Our team has developed an alternative protocol for postoperative pain management in pectus excavatum repair (Nuss procedure). While we recognize the established efficacy of continuous epidural techniques as the gold standard for such procedures, implementation in our country and workplace poses significant challenges. Our newest protocol integrates the use of epidural adjuvants such as dexmedetomidine and magnesium alongside a long-acting opioid (morphine). From Myron: Dr. Guardabassi is looking for help in studying and improving their protocol. If any of you could help his email address: guardabassidiego@hotmail.com
From Dr Mariconti Stefano, Bergamo, Italy
After reading today's interesting PAAD regarding analgesia in the Nuss procedure, I feel personally involved as we addressed exactly these issues at our center. Recently we published a paper that describes the successful transition from a TEA-based protocol to a Cryo one. [1]
Additionally we addressed the cryoanalgesia onset issue too, by placing the "cryo block" up to 6 days in advance, percutaneously, following Velayos et al. novel approach. [2] As a main result, we found that patients undergoing earlier cryo didn't require strong opioids postoperatively. Indeed, since percutaneous cryoanalgesia is performed by anesthesiologists...I believe this could be a valuable topic for open discussion!
1. Mariconti S. et al. Earlier preoperative percutaneous intercostal cryoanalgesia improves recovery after pectus excavatum surgery. Reg Anesth Pain Med. 2024 Nov 7:rapm-2024-105960. doi: 10.1136/rapm-2024-105960.
2. Velayos M, et al. Ultrasound-Guided Percutaneous Cryoanalgesia for Pectus Excavatum: When Should It be Applied? Eur J Pediatr Surg. 2023 Feb;33(1):61-67. doi: 10.1055/s-0042-1757361. Epub 2022 Oct 18. PMID: 36257335.