
Reader response
Myron Yaster MD

From Myron Yaster MD. This week we posted a PAAD Superretractors: The Virus of Research Misconduct and Fraud. Much to my chagrin, this is but the tip of the iceberg: Here is yet another example of research fraud from the Lancet. I will briefly review it and I’d like to thank Nancy Finnel and Mark Schreiner for sending me the PDF to review.
Original article
Topaz M, Roguin N, Gupta P, Zhang Z, Peltonen LM. Fabricated citations: an audit across 2·5 million biomedical papers. Lancet. 2026 May 9;407(10541):1779-1781. doi: 10.1016/S0140-6736(26)00603-3. PMID: 42107362.
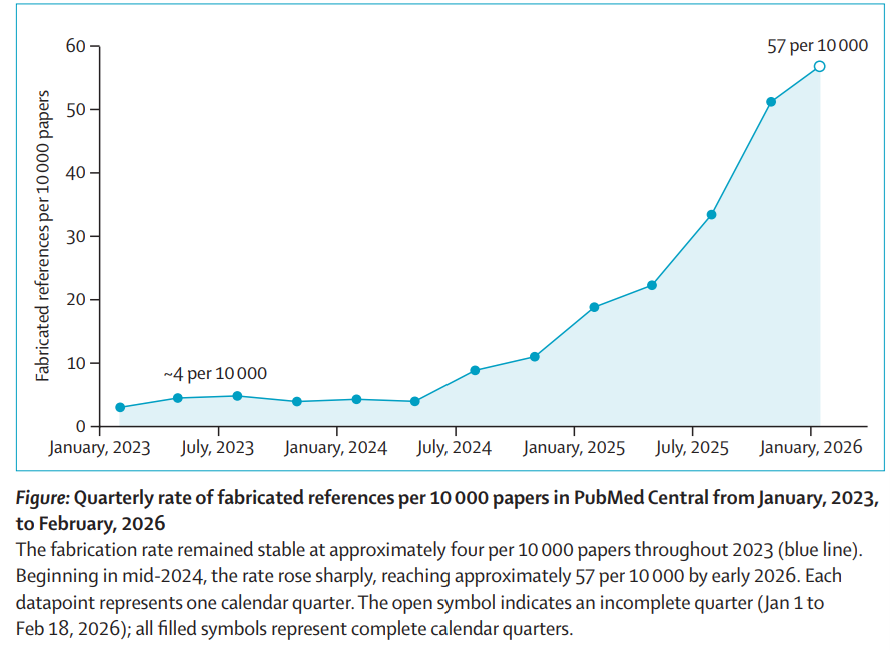
“Scientific literature depends on the integrity of its references. Each reference implicitly asserts that a verifiable source exists and supports the claims being made. When references point to non-existent studies, readers, reviewers, and policy makers are unable to evaluate the evidence.” Fabricated citations are emerging as a significant threat to the biomedical literature. This large-scale audit analyzed 2.47 million open-access biomedical papers (2023–2026) comprising 125.6 million references to quantify the prevalence and trajectory of fabricated citations.
Using an automated verification pipeline, references containing PubMed identifiers (PMIDs) were cross-checked against multiple databases, including PubMed, Crossref, OpenAlex, and Google Scholar. Advanced filtering methods, including large language model–assisted screening, were applied to distinguish true fabrications from formatting errors. Among 97.1 million verifiable references, 4,046 fabricated citations were identified across 2,810 papers, with a system precision of 91%.
The prevalence of fabricated citations increased sharply over time. In 2023, approximately 1 in 2,828 papers contained at least one fabricated reference; by early 2026, this rose to 1 in 277 papers, a more than 12-fold increase. Review articles demonstrated a 57% higher rate of fabrication compared with other publication types. Most affected papers contained one or two fabricated references, although some exhibited extensive fabrication patterns, including clusters suggestive of paper mill activity.
The temporal rise in fabricated citations coincides with widespread adoption of artificial intelligence writing tools like ChatGPT which generate plausible but fictitious references. Additional contributing factors include research misconduct (paper mills) and systemic gaps in peer review, where reference verification may not be routinely performed.
The implications are substantial. Fabricated citations undermine evidence synthesis, contaminate systematic reviews, and may ultimately influence clinical guidelines. Notably, over 98% of affected papers had not undergone correction or retraction at the time of analysis.
The authors recommend integrating automated reference verification into publication workflows, enhancing metadata transparency, and establishing formal tracking systems for fabricated citations. Routine verification represents a feasible and necessary intervention to preserve the integrity of the scientific record.
And one more thing. I am sure you are aware that we provide references in every PAAD. We obtain the references from citations within the articles we review. I use Pubmed to download the abstracts of each of these references to not only check if they actually exist but to be sure that the cited references accurately represent the original author’s conclusions.
From Mark Schreiner MD retired
In 2010 I was invited to give a talk about the medical advances portrayed in The Gross Clinic at The Philadelphia Museum of Art on the occasion of the painting’s restoration. https://www.philamuseum.org/exhibitions/an-eakins-masterpiece-restored-seeing-the-gross-clinic-anew I got the gig because my daughter was a curator at the PMA, not because I was in any way an expert but by the time I gave the talk, I was pretty knowledgeable. In 2011, I was asked to write a chapter for a book with the other speakers. Many of the things in my talk were secondary citations; I hadn’t read the originals of a number of important sources (e.g., Fanny Barney’s description of her mastectomy without anesthesia) For the chapter, I had to track down the original sources and turn in copies of any book, diary or journal article I cited; no secondary sources permitted. Thank goodness for Google Books and eBay. Without them I would never have found many of the original sources, many from the 1800’s. It was the most effort I ever expended ensuring all citations were accurate and real.
If a museum can demand such high standards for accuracy, can’t our journals do just a bit better too?
From George Gregory MD
Thank you for today’s PADD. You did not mention the massive effect these fraudulent papers can have on how some members of government use them to foster their belief in anti-vaccination. They can and do use them to support things like vaccinations cause autism. This can and does lead to massive harm. Look at measles recurrence.
From Richard Barnes, Staff Anaesthetist, Monash Children’s Hospital, Melbourne, Australia
Thanks for the excellent PAAD on a topic of great interest to me. A few thoughts:
It’s fortunate that neither Boldt nor Fujii et al were publishing on topics of major outcome-altering importance!
There are some important heroes here:
most importantly, Marcus and Oransky for setting up Retraction Watch
In the Fujii case, first Kranke and colleagues who were derided and ignored for a decade; then John Carlisle, whose painstaking manual statistical analysis proved the Fujii fraud beyond doubt
Steve Shafer, who has given a lot of thought to this topic in anaesthesia and how we might best respond to it
The situation is only going to get worse:
Peer review is becoming almost impossible
Paper mills, fake citations, etc
AI is and will be disastrous
Some (partial) solutions
Quality over quantity
Ignore citations
Eschew “publish or perish” mentality
Donate to Retraction Watch
From Matthias Koenig, MD, CHKD/CSG anesthesia group, Norfolk, VA
I believe the PAAD on perioperative antibiotics is a great reminder for all of us of an important topic, therefore thanks for putting it out there.
One aspect that I found surprising in the provided tables, however, was the listing of “alternative agents for beta-lactam allergic patients” for surgeries/procedures where cephalosporins were the primary drugs of choice. These recommendations are contradicted by current AAAAI publications (see link below). Apparently, the specter of cross reactivity is still alive ...
Years ago, at a different institution, our orthopedic colleagues experienced a significant increase of hardware infections in their posterior spinal fusion patients. A subsequent review by our infectious disease specialists identified the use of “alternative antibiotics” in patients claiming to be penicillin allergic as a culprit. This led to a change in institutional guidelines to administer cephalosporins whenever indicated except after documented anaphylactic reactions to penicillin. Going by the AAAAI info below, even that now appears over cautious.
https://www.aaaai.org/tools-for-the-public/latest-research-summaries/the-journal-of-allergy-and-clinical-immunology-in/2021/cephalosporins#
From Justin L. Lockman MD MSEd Children’s Hospital of Philadelphia
Thank you for the thoughtful articles about surgical antimicrobial prophylaxis. I have two thoughts about cefazolin and penicillin allergy that I wanted to share with PAAD readers. First, as you know there are many adults who have a history of “rash” after a dose of penicillin, particularly during childhood. This is often “true, true, and unrelated.” Because antimicrobials are so commonly prescribed inappropriately, many children with viral illness will receive antimicrobials and then later develop a rash from the virus. The classic example is roseola, where the rash usually occurs days after the fever starts.
Second and perhaps even more importantly, the classic “10% cross-reactivity” among beta lactam antimicrobials is misleading at best. The beta lactams have different side chains, and the side chains are responsible for the allergic reactions. Among drugs that share side chains (e.g., amoxicillin and cefadroxil) there some risk (20-40%) of reaction. But among drugs without the same side chain (note that cefazolin has absolutely no shared side chains with any penicillin or cephalosporin for sale in the US), there is NO risk of cross reactivity. Indeed, for rare patients who happen to have allergy to cefazolin in the setting of known other beta lactam allergy, it is almost certainly a second, unrelated hypersensitivity/allergy. For more information on this topic, see this website (https://www.idstewardship.com/wp-content/uploads/2017/06/Beta-lactam-side-chain-handout-6.26.2025.pdf) or any other of a number of publications with beta lactam side chain tables published in the past 10 years.