


POCUS and Aeration heterogeneity in neonates and how it may vary with different respiratory disorders
Christopher B. Massa MD PhD and Anthony Alexander MD

Admittedly I’ve always been interested in pulmonary physiology. Indeed, the application of respiratory physiology to clinical practice was one of the driving forces that drove me to become an anesthesiologist. So when I saw today’s article1 and its accompanying editorial2 I thought “WOW” this will be a great PAAD. Of course, as I read these articles, which are based on the use of POCUS to visualize aeration heterogeneity in neonates with different respiratory disorders I realized immediately that I knew nothing about these issues and needed a guide in the wilderness! Fortunately for me, and for you, I found Dr. Christopher Massa, an Assistant Professor of Anesthesiology and Critical Care at the Children's Hospital of Philadelphia to help! Myron Yaster MD
Original article
Loi B, Sartorius V, Vivalda L, Fardi A, Regiroli G, Dellacà R, Ahsani-Nasab S, Vedovelli L, De Luca D. Global and Regional Heterogeneity of Lung Aeration in Neonates with Different Respiratory Disorders: A Physiologic Observational Study. Anesthesiology. 2024 Oct 1;141(4):719-731. doi: 10.1097/ALN.0000000000005026. PMID: 38657112.
Editorial
Sett A, Dahm SI, Tingay DG. Lung Ultrasound and Regional Heterogeneity: A Bedside Solution to an Underrecognized Problem? Anesthesiology. 2024 Oct 1;141(4):635-637. doi: 10.1097/ALN.0000000000005136. PMID: 39254536.
Mechanical ventilation is a cornerstone in the management of critically ill neonates in the intensive care unit and operating room. The idea that mechanical ventilation can cause pulmonary injury, and consequently the quest for strategies to mitigate that risk, has existed for almost as long as the technology of mechanical ventilation itself. We are all familiar with the various mechanisms of ventilator-induced lung injury – volutrauma (overdistension), barotrauma (high alveolar and airway pressures) and atelectotrauma (cyclical closing and opening of the alveoli) – all of which culminate in inflammatory injury to the lung.3 The respiratory anatomy and physiology of neonates makes them more susceptible to these mechanisms of injury. Their airways are smaller and more complaint predisposing them to higher airway resistance and a propensity for airway collapse. Decreased number of alveoli and a highly compliant thorax predisposes them to atelectasis.4 Less compliant lungs require higher inflating pressures to produce adequate tidal volumes. It seems intuitive that lowering volumes, reducing ventilating pressures, and applying sensible positive end expiratory pressure (PEEP) would reduce each of these mechanisms of injury. Indeed, the Acute Respiratory Distress Network (ARDSNet) provided landmark evidence that lower tidal volumes and higher positive PEEP reduces ventilator-induced lung injury (VILI) and mortality in adults with acute respiratory distress syndrome.5
Since then, we’ve realized that the relationship between lung volumes and VILI is a little more complicated than that. Within different regions of the lung, atelectasis and overdistension can coexist as parallel mechanisms for injury. The global and regional aeration state of the lung, not just the total volume determines the severity of VILI. In the almost twenty-five years since ARDSNet, point-of-care ultrasound (POCUS) has become a ubiquitous tool in the ICU and operating room. Can we use ultrasound to better understand lung aeration and to perhaps reduce the risk of VILI in neonates? Today’s PAAD examines a study by Loi et al.,1 which describes a novel use of lung ultrasound to measure aeration heterogeneity in different disease states in mechanically ventilated neonates.
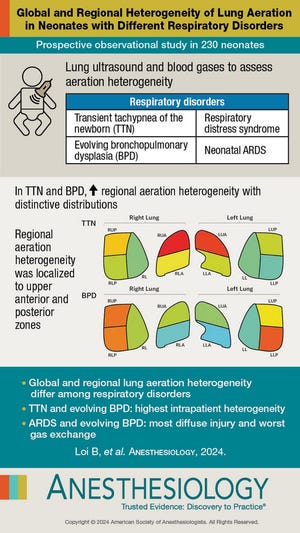
In this study, 246 infants were examined using quantitative lung ultrasound across 10 lung regions to assess ventilation distribution in healthy neonates and those with lung disease (see visual abstract image above). This was a prospective study enrolling 16 neonates with no lung disease as well as 50 infants each meeting established diagnostic criteria for respiratory distress syndrome (RDS), transient tachypnea of the newborn (TTN) and evolving bronchopulmonary dysplasia (BPD), as well as 80 neonates with neonatal acute respiratory distress syndrome (NARDS). NARDS patients were further stratified as mild (6 patients), moderate (20) and severe (54). The primary hypothesis of this study was that characteristic patterns of ventilation distribution and degree of heterogeneity were differentiable by etiology of respiratory failure. As a secondary endpoint, this study also proposed that ventilation heterogeneity correlated with measures of impaired gas exchange (transcutaneous pCO2 and pO2). Excluded from the study population were infants with complex congenital malformations or known chromosomal abnormalities, congenital lung abnormalities, presence of pneumothorax, pneumomediastinum or plural effusions interfering with imaging or the need for thoracic surgery. There were some demographic differences between the causes of respiratory failure, as to be expected: children with RDS or BPD had younger gestational age at birth and birth weight compared to NARDS, TTN and obviously healthy neonates. Patients with NARDS and BPD had higher mean airway pressure requirements (pooled CPAP and mechanical ventilator). Of note, lung ultrasound was only performed by skilled clinicians with at least 3 years of neonatal lung ultrasound experience ! Each hemithorax was divided into 5 regions (anterior upper/lower, posterior upper/lower and lateral) and given a defined score from 0-3 based on imaging findings:
0: Class A - Normal aeration with A-lines only
1: Class B - Alveolar-interstitial with >3 well spaced B-lines
2: Class B Severe - Crowded, coalescent B-lines
3: Class C - Consolidation. Mixed hypo- and hyperechogenic areas with irregular borders and size greater than 1 cm
The study’s primary endpoints were to measure the global and regional lung heterogeneity in each cause of respiratory failure. Global heterogeneity within each patient was assessed by calculating the coefficient of variation (standard deviation divided by mean) of the ultrasound scores across all 10 measurement windows. Heterogeniety across patients with the same respiratory disorder was assessed by computing the Gini-Simpson index, which quantifies the diversity of all measurements made in that condition; this index ranges from 0 to 1, with higher numbers indicating greater population heterogeniety. Regional heterogeneity in each cause of respiratory failure was estimated by calculating the coefficient of variation of each lung region across all patients measured. In addition, total lung aeration was evaluated by computing an “extended lung ultrasound score”, which was the sum of all 0-3 scores across the 10 lung regions for each patient. Secondary endpoints assessing ventilation efficacy included oxygenation index, A-a gradient, and the ratios of Arterial/alveolar PO2, Arterial PO2/FiO2 and SpO2/FiO2.
Global heterogeneity as determined by coefficient of variation in the healthy neonate was expectedly very low at 1.6 +/- 1%, which is unsurprising using this metric, as the lung should normally consist of A -lines with rare B-lines. High degrees of heterogeneity characterized all causes of lung injury, with TTN and BPD patients showing an average of ~60% heterogeneity, with RDS around 40% and NARDS near 25%, each with fairly significant variance in the population. The global inter-patient heterogeneity evaluated by the Gini-Simpson index was 0.3 in the healthy group, and elevated in each pathology with BPD (0.7), TTN (0.62), and NARDS (0.6) being higher than RDS (0.5). Next the authors showed what percentage of the measured regions had each score from 0 to 3. Unsurprisingly, the NARDS group had the most consolidated lung regions (50%!) and also the fewest healthy lung (1%). RDS showed very little consolidated lung (2.0%), but also very little class A lung (4.6%). The patterns observed in the most heterogeneous pathologies were unique: TTN contained a sizable proportion (18%) was healthy lung, with few regions of consolidation (2.4%) with the remainder being class B/B-severe, while evolving BPD showed 15% consolidated lung, and 14% healthy lung! I think it suffices without saying, I just want to pause a moment to say these are VERY different lungs! The implications of this heterogeneity on ventilation distribution and the risk of (or result of) regional overdistension injury are very significant. If this interests you, I implore you – pictures are worth 1000 words. Look at Figures 1C and 2 in the journal (below).


The secondary endpoints in this study relate global heterogeneity to measures of ventilation, aeration and oxygenation using regression analysis. The important take home messages are that increasing heterogeneity is associated with IMPROVED aeration (lower extended lung ultrasound score), and all measured oxygenation indices. While the strength of this association and the specific regression coefficients vary based on etiology, it is a consistent finding across all 4 conditions.
But wait, you say! Isn’t heterogeneity bad? In this study it seems to be a proxy for healthy lung, or at the very least, lung tissue that is less flooded/atelectatic and relatively compliant. While heterogeneity is often equated as a measure of pathology, it should be noted that uniformly consolidated lung will be full of disease, but there will be little heterogeneity. Also, lung that has areas of focal consolidation and areas of normal lung may have a lower mean heterogeneity, but have much more variation within each subject. In either case, I think its helpful to think of heterogeneity in this sense as a measure of the degree of at-risk lung for injurious ventilation.
So, what’s the take home? Lets say you’re awesome at performing point of care ultrasound - can you use this in the OR today? Well… if you can, please let us know! This is certainly a fantastic study that develops a technique with great potential to evolve toward less injurious initial ventilator settings for different etiologies of neonatal respiratory failure, monitoring progression vs recovery of lung function in neonates and risk stratification for individual patients. So far as I see it, there are several factors which would limit its utility intraoperatively, notably that its not a continuous monitor and is spatially constrained, requiring frequent resampling across the thorax. But also it defines heterogeneity using consolidation and interstitial fluid, which, while certainly correlated with mechanical dysfunction have an unclear translation to guide any changes in respiratory support. It may have utility as a PEEP titration tool to reduce regional or global heterogeneity with recruitment, however compliant regions will still preferentially receive dynamic flow, while highly consolidated ones will be more PEEP refractory. Harkening back to our first paragraph, were uncertain that awareness of mechanical heterogeneity actually helps us prevent regional overdistension within our current approach to managing ventilation. Much work remains to be done in the field of ventilation optimization in the sick neonate, but we’re hopeful this foundational work will advance the field.
Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Loi B, Sartorius V, Vivalda L, et al. Global and Regional Heterogeneity of Lung Aeration in Neonates with Different Respiratory Disorders: A Physiologic Observational Study. Anesthesiology 2024;141(4):719-731. (In eng). DOI: 10.1097/aln.0000000000005026.
2. Sett A, Dahm SI, Tingay DG. Lung Ultrasound and Regional Heterogeneity: A Bedside Solution to an Underrecognized Problem? Anesthesiology 2024;141(4):635-637. (In eng). DOI: 10.1097/aln.0000000000005136.
3. Angurana SK, Sudeep KC, Prasad S. Ventilator-induced lung injury in children. Journal of Pediatric Critical Care 2023;10(3):107-114. DOI: 10.4103/jpcc.jpcc_27_23.
4. Neumann RP, von Ungern-Sternberg BS. The neonatal lung – physiology and ventilation. Pediatric Anesthesia 2014;24(1):10-21. DOI: https://doi.org/10.1111/pan.12280.
5. Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The New England journal of medicine 2000;342(18):1301-8. (In eng). DOI: 10.1056/nejm200005043421801.