


Placental Abnormities and the Development of Congenital Heart Disease (CHD) : Therapeutic Target or Immutable Component?
James DiNardo, Viviane Nasr, Lindsey Loveland, Susan Nicolson

Original article
Josowitz R, Ho DY, Shankar S, Mondal A, Zavez A, Linn RL, Tian Z, Gaynor JW, Rychik J. Congenital Heart Disease Fetuses Have Decreased Mid-Gestational Placental Flow, Placental Malperfusion Defects, and Impaired Growth. JACC Adv. 2025 Jan 16;4(2):101559. doi: 10.1016/j.jacadv.2024.101559. PMID: 39898349; PMCID: PMC11786062.
In a previous PAAD (June 12, 2023 Impairments to the Maternal-Fetal Environment Can Impact Risk For Postnatal Preoperative White Matter Brain Injury: Issues Prior To Ex-Utero Therapies: https://ronlitman.substack.com/publish/posts/detail/126887843?referrer=%2Fpublish%2Fposts%3Fsearch%3DMaternal-Fetal%2520Environment our group reviewed a study that delineated the association between an impaired maternal-fetal environment (MFE) and infant white matter injury (WMI) prior to infant cardiac surgery.1 Increasing risk for preoperative WMI was associated with male sex, impaired MFE, longer time from birth to surgery and preoperative brain maturation. Impaired MFE was defined by the self-reported presence of ≥1 of the following: gestational hypertension, preeclampsia, gestational diabetes, and/or maternal smoking during pregnancy.
The key component of the MFE is the placenta. Its role in the development of CHD is particularly important given that the majority of CHD is not explained by identifiable genetic or environmental factors. It is well established that the heart and placenta develop concurrently, with heart tube specification occurring at days 16–21 and a rudimentary villous tree forming by day 21 of gestation.2 Heart and placental development share common regulatory pathways. Cardiomyocyte specification and extra villous trophoblast invasion are both regulated by Notch and Wnt.3 The endocardial cushion develops from neural crest cells to form heart valves and septa and requires the same genes as the placenta for proper formation and remodeling.
A group at the Children’s Hospital of Philadelphia (CHOP) demonstrated decreased mid-gestational umbilical vein venous volume flow (UVVF) parameters in CHD fetuses compared to controls. In their most recent work, they sought to determine whether CHD fetuses with impaired placental blood flow demonstrate distinct pathological features of the placenta at birth.4 A case-control study was conducted with a total of 38 fetal cases, the majority with single ventricle (SV) CHD, compared with 36 fetal controls. Control subjects were recruited from referrals due to clinical indications for screening fetal echocardiograms, and as the authors acknowledge, may not fully represent low risk, normal pregnancies. The median gestational age of the cases was slightly higher than those of the controls (23 weeks vs 21 weeks; P < 0.001). Maternal age was slightly lower in cases compared to controls. There was no difference in the distribution of maternal race, comorbidities, medication exposure, or fetal sex between cases and controls. While only present in few subjects, there was no difference in prevalence of maternal hypertension, preeclampsia, or maternal aspirin use between groups.
As a component of a fetal echocardiographic exam, the umbilical vein was visualized in a free loop in the longitudinal plane and 3 measurements of the diameter of the vessel were averaged. Spectral Doppler of the umbilical vein was obtained at an angle of insonation of <20°. Due to the laminar flow pattern in the umbilical vein, the mean velocity is equal to half the maximum velocity. The cross-sectional area of the umbilical vein multiplied by the mean velocity of flow yields the rate of blood flow, UVVF, in mL/min. All placentas were examined in the pathology department at CHOP utilizing a systematic protocol, including recording the trimmed placental weight, membrane insertion, gross appearance, dimensions of the placental disc, and umbilical cord characteristics. Histologic samples included sections of membranes, umbilical cord, and at least 3 full-thickness sections of non-lesion placental parenchyma. Macroscopic and microscopic lesions were described according to standardized criteria.
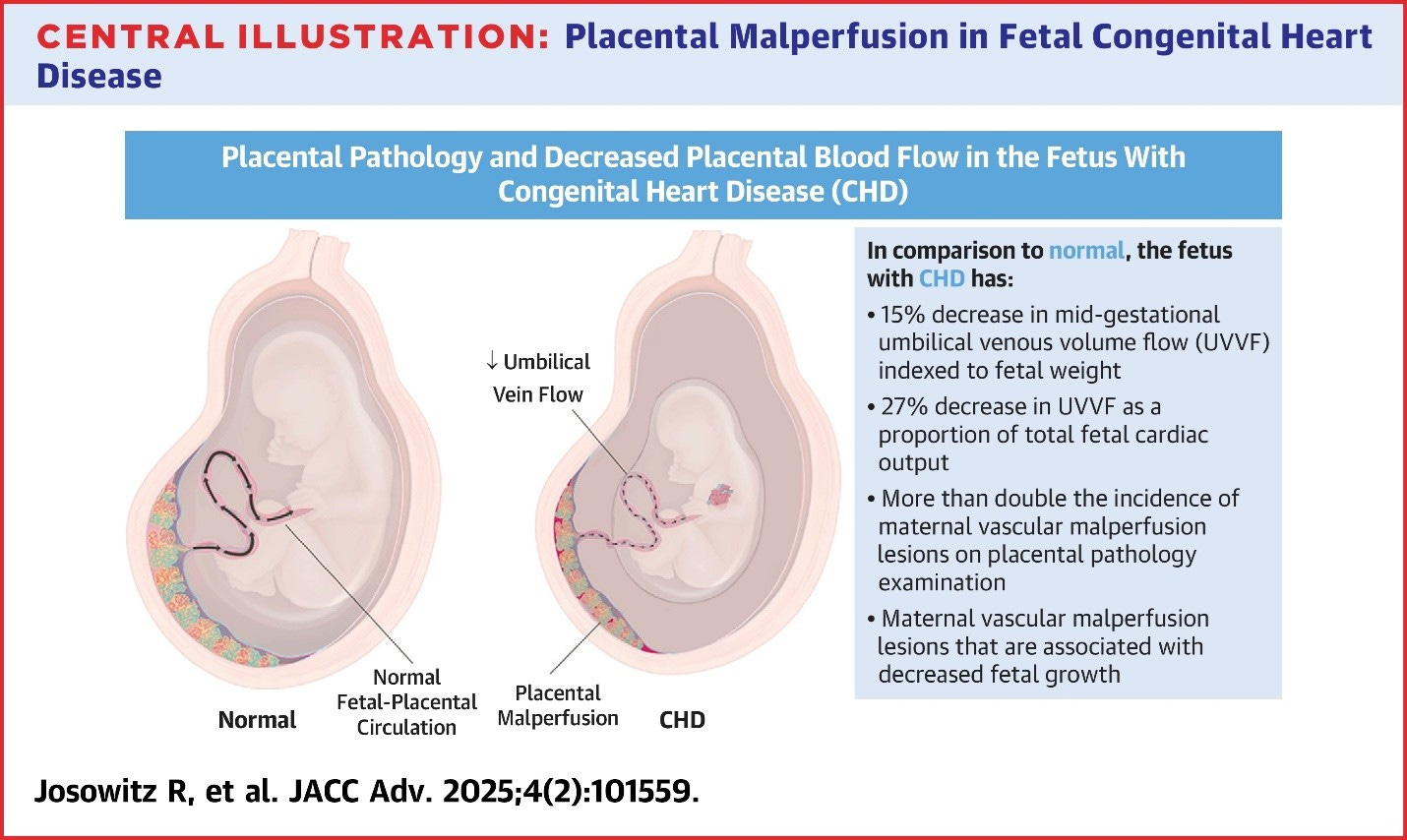
CHD fetuses had a 15% decrease in mid-gestational UVVF indexed to fetal weight (P < 0.01), and a 27% reduction in UVVF as a proportion of fetal cardiac output (P < 0.01) compared to controls. Stated differently, CHD fetuses had on average only 22% of fetal CCO returning from the placenta as compared to the normal 30%. The authors hypothesized that this may be due to increased placental resistance. CHD fetuses had increased placental maternal vascular malperfusion (MVM) lesions (44% vs 18%, P < 0.05), especially high-grade MVM (39% vs 9.1%, P . 0.05), and a trend toward increased placental fetal vascular malperfusion lesions (42% vs 23%, P . 0.10). Placental MVM but not fetal vascular malperfusion lesions were associated with decreased birth weight in CHD fetuses (P < 0.001). However, there was no difference in the prevalence of other placental abnormalities between groups, including umbilical cord abnormalities, chronic inflammation, increased villous vascularity, or other significant pathology such as massive perivillous fibrin deposition, delayed villous maturation, or chorangiosis (see figure).
This study proves to be another interesting piece of the puzzle regarding placental malperfusion (PMP) defects, their association with development of CHD, and the contribution of these defects to tangible outcomes in children with CHD. It remains to be seen whether placental abnormalities are a potential site of meaningful interventions or an immutable developmental component of CHD.
Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Licht DJ, Jacobwitz M, Lynch JM, et al. Impaired Maternal-Fetal Environment and Risk for Preoperative Focal White Matter Injury in Neonates With Complex Congenital Heart Disease. J Am Heart Assoc 2023;12(7):e025516. (In eng). DOI: 10.1161/jaha.122.025516.
2. Courtney JA, Cnota JF, Jones HN. The Role of Abnormal Placentation in Congenital Heart Disease; Cause, Correlate, or Consequence? Front Physiol 2018;9:1045. (In eng). DOI: 10.3389/fphys.2018.01045.
3. Acar A, Hidalgo-Sastre A, Leverentz MK, et al. Inhibition of Wnt signalling by Notch via two distinct mechanisms. Sci Rep 2021;11(1):9096. (In eng). DOI: 10.1038/s41598-021-88618-5.
4. Josowitz R, Ho DY, Shankar S, et al. Congenital Heart Disease Fetuses Have Decreased Mid-Gestational Placental Flow, Placental Malperfusion Defects, and Impaired Growth. JACC Adv 2025;4(2):101559. (In eng). DOI: 10.1016/j.jacadv.2024.101559.