


Perioperative Anxiety Assessment Tools
Romy Yun, M.D.

Original article
Yun R, Caruso TJ. Identification and Treatment of Pediatric Perioperative Anxiety. Anesthesiology. 2024 Nov 1;141(5):973-983. doi: 10.1097/ALN.0000000000005105. PMID: 39163600.
Hospitalized children experience significant anxiety. Perioperatively, the fear of parental separation, unfamiliar healthcare providers, and an unknown environment compound feelings of distress. Immediate effects of preoperative anxiety are often observed intraoperatively and in the recovery room.1 However, impacts to the patient and family extend beyond the postoperative period. Long term side effects such as post-traumatic stress symptoms, and sleep disturbances may perpetuate for months as well as fear of medical settings into adulthood.1,2
One of the earliest formal characterizations of perioperative anxiety was based on the modified Yale Preoperative Anxiety Scale (mYPAS).3 Used in over a hundred studies, the scale contains five domains (activity, vocalization, emotional expressivity, state of apparent arousal, and use of parents) measured over four timepoints.3 While the scale possesses high validity and reliability, its complexity, need for prior training, and time required to complete impede its clinical use.
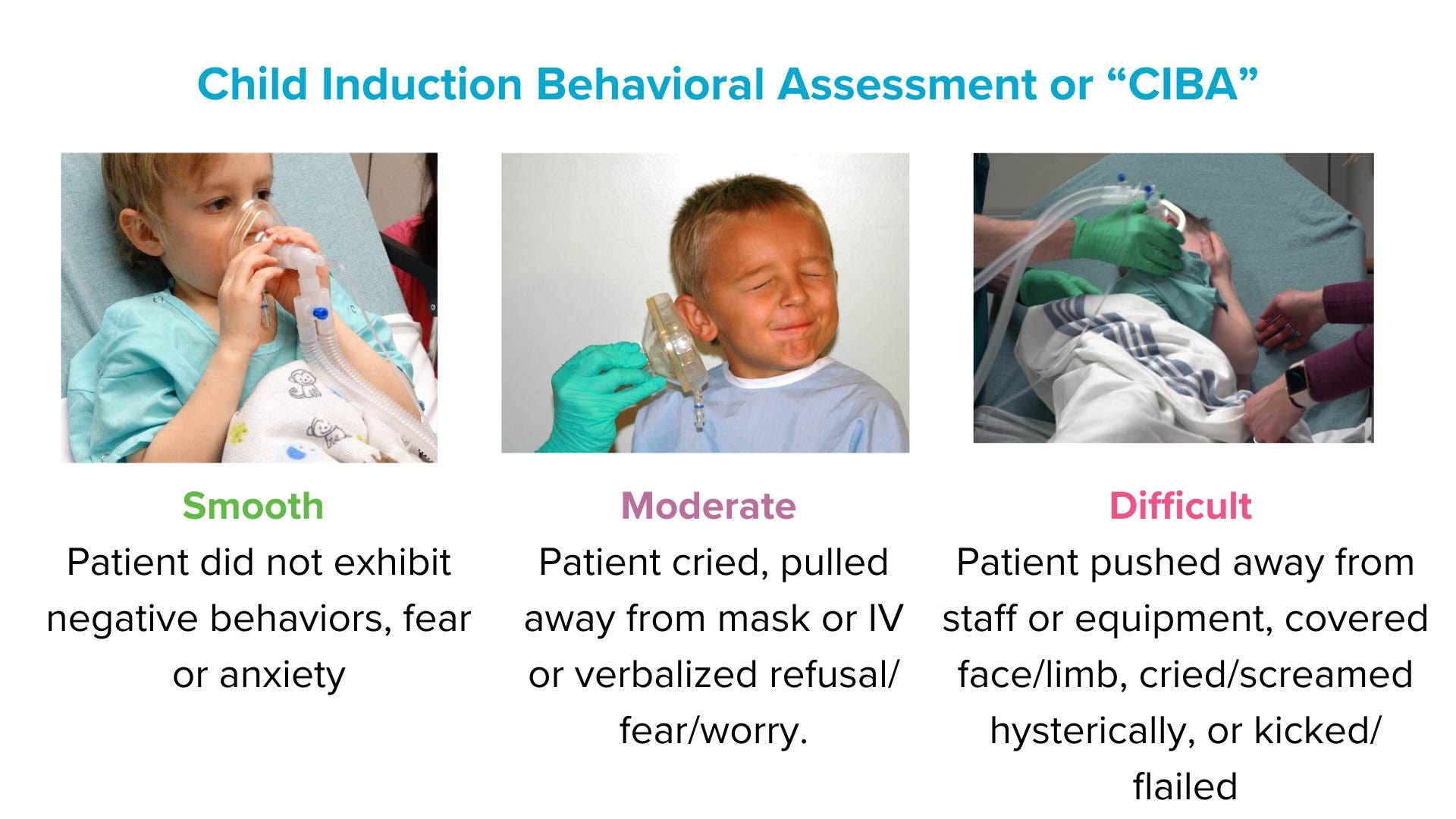
Routine perioperative anxiety identification requires an intuitive and facile assessment scale. One clinical affect assessment widely integrated into the EPIC electronic medical record (EMR) is the Childhood Induction Behavioral Assessment (CIBA).4,5 The CIBA scale is scored by selecting one of three categories, each containing several descriptors of various levels of affect, behavior, and cooperation specific to anesthesia induction.4,5 Although CIBA is commonly used in its standard default EPIC integration, the scale itself lacks internal validity. Additionally, its categories include multiple descriptors that may convey varying meanings due to the merging of affect, behavior, and cooperation. For instance, a cooperative but anxious child may have differing clinical implications compared to an uncooperative but happy child.

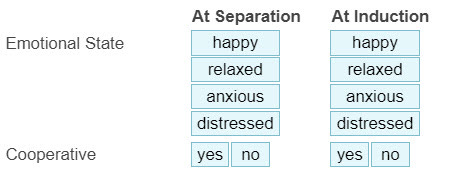
The Happy, Relaxed, Anxious, and Distressed with yes/no to cooperation (HRAD±) scale is an observational scale with common and intuitively known affects with a distinct cooperation score.6,7 With affect and cooperation as separate constructs, the scale has demonstrated strong correlations to mYPAS and other validated research scales as well as good reliability with multi-level providers.6–9 In addition to its utility as an assessment scale during induction of anesthesia, HRAD± has been studied internationally and used to rate procedural distress during vascular access procedures.6–9 Currently, HRAD± can be added to enhance existing EPIC documentation, and the EPIC steering committee is exploring its integration into the foundation system.
With increasing EMR utilization and potential for large scale, population-based outcomes research, a standardized assessment tool for the identification of pediatric perioperative anxiety is vital. HRAD± is an intuitive scale that has been studied with nursing, anesthesiology, and vascular access providers within both perioperative and acute care patients in the United States and abroad. HRAD± provides a reliable and well-studied scale to guide targeted interventions. Future endeavors should prioritize ideal scale standardization for the reliable identification and treatment of pediatric perioperative anxiety to minimize postoperative complications and improve future encounters.10
Are you using anxiety scales in your practice? Please send your experiences with these scales to Myron and any other comments and he will post in a Friday reader response.
References
1. Kain ZN, Mayes LC, O’Connor TZ, Cicchetti DV. Preoperative Anxiety in Children: Predictors and Outcomes. Arch Pediatr Adolesc Med. 1996;150(12):1238-1245. doi:10.1001/archpedi.1996.02170370016002
2. Lerwick JL. Psychosocial implications of pediatric surgical hospitalization. In: Seminars in Pediatric Surgery. Vol 22. Elsevier; 2013:129-133.
3. Kain ZN, Mayes LC, Cicchetti DV, Bagnall AL, Finley JD, Hofstadter MB. The Yale Preoperative Anxiety Scale: How does it compare with a “gold standard”? Anesth Analg. 1997;85(4):783-788. doi:10.1097/00000539-199710000-00012
4. Winterberg AV, Colella CL, Weber KA, Varughese AM. The Child Induction Behavioral Assessment Tool: A Tool to Facilitate the Electronic Documentation of Behavioral Responses to Anesthesia Inductions. J Perianesth Nurs. 2018;33(3):296-+. doi:10.1016/j.jopan.2016.10.004
5. Winterberg AV, Ding L, Hill LM, Stubbeman BL, Varughese AM. Validation of a Simple Tool for Electronic Documentation of Behavioral Responses to Anesthesia Induction. Anesth Analg. 2020;130(2):472-479. doi:10.1213/ANE.0000000000003945 [doi]
6. Kennedy K, Wang E, Rodriguez ST, et al. Development and assessment of an efficient pediatric affect and cooperation scale. J Clin Anesth. 2022;76:110569.
7. Yun R, Qian D, Wang E, et al. A prospective, observational validation of HRAD±, a novel pediatric affect and cooperation scale. J Clin Anesth. 2024;94:111410.
8. Connell J, Anito M, Kageha E, et al. Preoperative Distraction using Virtual Reality in Resource Variable Settings. Accepted in Southern African Journal of Anaesthesia and Analgesia.
9. Yun R, Kennedy K, Titzler J, et al. A Prospective, Observational Study of a Pediatric Affect and Cooperation Scale (HRAD±) for Vascular Access Procedures. Accepted in Journal of Vascular Access.
10. Yun R, Kennedy KM, Caruso TJ. Perioperative Pediatric Anxiety: A Cry for Universal Scale Adoption. Pediatr Qual Saf. 2022;7(2).