
Perioperative anaphylaxis
Myron Yaster MD and Lynne G. Maxwell MD

25 + years ago while providing general anesthesia to a child with spina bifida undergoing a posterior spinal fusion in the prone position, an intraoperative, near miss catastrophe occurred. The child became suddenly acutely hypotensive and hypoxemic. Routine measures like giving fluid, turning down the vapor anesthetic, increasing the FiO2 to 100% did nothing, and fearing an imminent cardiac arrest, I declared an emergency, called for help, asked the surgeon to quickly close and turned the patient to the supine position. Once supine and as the lines and monitors were untangled and reconnected, I started an epinephrine infusion and almost immediately and miraculously everything returned to normal. Our diagnosis? The recently (at the time) described phenomenon of latex allergy/anaphylaxis. Interestingly, we decided to proceed with surgery thinking that since all of the mast cells had degranulated no further release and circulatory compromise would occur. Indeed, the case was completed uneventfully, with continuation of the epinephrine infusion. On the other hand, the near miss resulted in a root cause analysis and resulted in removal of all, or almost all, latex containing products from the hospital. Additionally, another result of the root cause analysis was a discussion and practice sesssions of how to do CPR in the prone position.
The subject of today’s PAAD is an excellent review of perioperative anaphylaxis. Interestingly to me, the one action item in the review’s discussion that is not mentioned and should be is to open SPA’s Pedi Crisis version 2 app. Almost all of the diagnostic, differential diagnosis, and treatment options discussed in the article can be found in the app. So for new readers, if you haven’t downloaded the app from the iOS or Android stores or from SPA’s website, do it now! Myron Yaster MD
Original review article
Tacquard C, Iba T, Levy JH. Perioperative Anaphylaxis. Anesthesiology. 2023 Jan 1;138(1):100-110. PMID: 36413685
During anesthesia we administer a variety of drugs, blood products and/or imaging agents that potentially can cause anaphylaxis, that is, an immediate hypersensitivity reaction. Diagnosing anaphylaxis in anesthetized patients may be difficult. Many of the classic signs and symptoms like urticaria, pruritus, erythema, facial swelling, loss of consciousness may be undetectable in anesthetized patients. Acute hypotension, bronchospasm, and hypoxemia can easily be confused with other more common intraoperative events like excessive anesthesia, an endotracheal tube tickling the airway, pulmonary edema, aspiration, transfusion related acute lung injury (TRALI), air embolism, sepsis, etc.
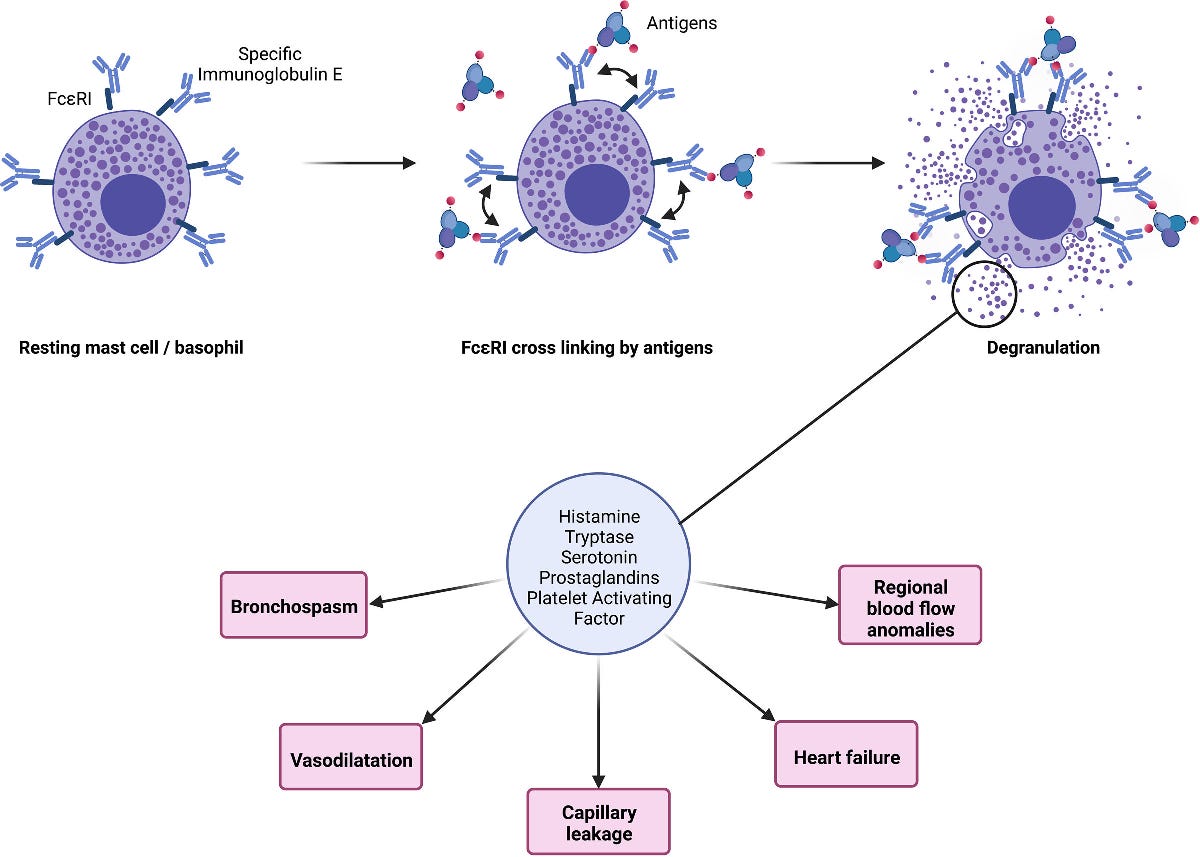
What causes anaphylaxis? The massive release of multiple physiologically active mediators by inflammatory cells. “In immunoglobulin E–mediated anaphylaxis, the mechanism most frequently encountered in the perioperative setting, mast cells and basophils are the main cells involved. (Figure) However, the immunoglobulin E–mediated mechanism is identified in only about 60% of perioperative anaphylaxis, which raises the question of other mechanisms involved, including immunoglobulin G–mediated reactions or complement activation. Previously, non-immunoglobulin E–dependent reactions were called anaphylactoid, but this term is no longer used. The term anaphylaxis refers to the clinical presentation but not the mechanism”.1
The drugs that most commonly produce anaphylaxis are antibiotics (penicillins, cephalosporins, glycopeptides), neuromuscular blocking agents (succinylcholine, rocuronium) dyes (particularly patent blue V (used for sentinel node identification)), sugammadex, and chlorhexidine. Interestingly, where you live is important. In the U.S. and the U.K. antibiotics are the most common triggers, whereas in Europe, the neuromuscular blocking agents are most common.
The key to clinical management is early recognition and prompt cardiopulmonary resuscitation with epinephrine, to counteract the associated massive vasodilation and myocardial dysfunction. Although not stated in the article: DO NOT RELY ON YOUR MEMORY! Open the Pedi Crisis app, declare an emergency, call for help and immediately increase the FiO2 to 100%. We’ve synthesized the article’s recommendations and the app’s treatment plan.
· Remove the triggering agent if possible (think latex) or stop the administration of the suspected allergen. Call for help.
· Maintain ventilation with 100% oxygen. Consider intubation if not already intubated.
· Give an epinephrine bolus (1-19 mcg/kg) and start an infusion (0.02-1 mcg/kg/minute). Epinephrine infusion may need to be continued after completion of surgery, and the patient may require intensive care.
· Restore intravascular volume with 10-30 mL/kg normal saline or Ringers Lactate given rapidly.
· For refractory hypotension, give vasopressin 10 milliunits/kg IV.
· To treat severe bronchospasm, consider nebulized albuterol, although IV epinephrine is preferred.
· To decrease mediator release and help in the early post resuscitation period consider methyl prednisolone 1-2 mg/kg (maximum 100 mg).
· The app suggests giving diphenhydramine 1 mg/kg (max 50 mg)and or famotidine 0.25 mg/kg (max 20 mg) to reduce histamine related effects. The article does not.
· Draw blood for a tryptase level best collected at least 30 minutes to 2 (or 3) hours after the event to help confirm the diagnosis of mast cell activation.
Whether to proceed with surgery after a reaction is unclear and debatable. Finally, if perioperative anaphylaxis is suspected, European guidelines suggest the patient should be referred to an allergist. The allergy consultation should be scheduled at least 6 weeks after the suspected anaphylaxis event, to avoid false-negative skin tests due to mast cell granule depletion. Because provocation tests using anesthetic agents involve a high level of risk for the patient, the allergy workup is mainly based on skin tests (skin prick test and intradermal reactions) using different nonirritating drug concentrations validated on a cohort of healthy volunteers, although some immunoglobulin E assays have been developed for some of the drugs/subtances of interest (lates, neuromuscular blocking agents, thiopental, chlorhexidine, penicillin). At the conclusion of allergy evaluation, the drug responsible for the reaction may not be identified in 40% of the cases.
PS from Lynne who although a bit older than Myron has a far better memory. “The first case of latex anaphylaxis that we saw at Hopkins was a patient with bladder exstrophy being operated on by the late Dr. Bob Jeffs. Dr. Charlie Schleien was the attending anesthesiologist. The patient had had an IJ central line placed and it was thought that maybe the hypotension was from the line placement (vessel or atrial injury). The case was canceled and the patient came back a few weeks later. No central line was placed but the hypotension recurred around 20 minutes after incision. Then Jim Robotham (who died last year) remembered the NEJM article about latex anaphylaxis he had read. Interestingly, before we eliminated latex from the OR and hospital environment, Dr. Jeffs started to operate with vinyl gloves and actually did one surgery without gloves!!”
References
1. Tacquard C, Iba T, Levy JH. Perioperative Anaphylaxis. Anesthesiology. Jan 1 2023;138(1):100-110.