


Pediatric anesthesiology fellows: an endangered species?
Myron Yaster MD, Justin L. Lockman MD, MSEd, Aditee Ambardekar MD, M. Concetta Lupa, MD and Anisha Nadkarni MD

Although the number of trainees finishing anesthesiology residency programs continues to increase, the percentage of graduates going into pediatric anesthesiology subspecialty training programs has decreased. Indeed, even accounting for the recent overexpansion of training program positions in pediatric anesthesia, 67% of pediatric anesthesiology training programs (and 36% of positions) did not fill in the match in October 2022 because fewer graduates pursued training and careers in pediatric anesthesiology. The growth of positions offered in pediatric anesthesia has continued to outpace the growth rate of applicants as pointed out by Cladis et al.1, and the number of matched fellows in pediatric anesthesia actually decreased to 137 for this past match from the usual 180-200. Importantly, while some have speculated that COVID-related salary changes have affected the number of applicants to subspecialty fellowship programs, this divergence is NOT mirrored across other anesthesiology subspecialty training programs.
Taking this one step further, the pipeline to pediatric cardiac anesthesia has now been seriously disrupted, and some centers (and most importantly, their patients) are suffering from a shortage of experts in this area. We’ve seen this happen before…just take a look at pediatric critical care. Anesthesiologists by and large have abandoned this profession, a field of medicine they created.2 Extending training duration seems simply not to be worth it to many new graduates. Some of you may recall a national discussion about adding a second year to pediatric anesthesia training over the past decade; this idea has now been completely abandoned (for those who were worried about it!) in exchange for more rigorous training during the pediatric fellowship year – more to come about that process in a future PAAD.
What this means and how it will affect our profession in the near and long term is very concerning and the editors of the PAAD will keep our eyes open for articles that address some of these issues. Our friends and colleagues in PEDIATRICS have been dealing with this problem for a while. My best friend, Dr. David Nichols, a pediatrician and anesthesiologist, and the former president of the American Board of Pediatrics, pointed me to some papers on this topic in the Pediatric literature, which we will review in today’s PAAD. I’ve asked Drs. Lockman, Ambardekar, Lupa and Nadkarni, all of whom are deeply involved in the Pediatric Anesthesiology Program Directors’ Association and the SPA Trainee Special Interest Group to assist. Myron Yaster MD
Original articles
Eva Catenaccio, Jonathan M Rochlin, Harold K Simon. Association of Lifetime Earning Potential and Workforce Distribution Among Pediatric Subspecialists. JAMA Pediatr. 2021 Oct 1;175(10):1053-1059. PMID: 34180976 3
Jonathan M Rochlin and Harold K Simon. Does fellowship pay: what is the long-term financial impact of subspecialty training in pediatrics? Pediatrics. 2011 Feb;127(2):254-60. PMID: 21262882 4
Eva Catenaccio, Jonathan M Rochlin, Harold K Simon. Differences in Lifetime Earning Potential for Pediatric Subspecialists. Pediatrics. 2021 Apr;147(4):e2020027771. PMID: 33685988 5
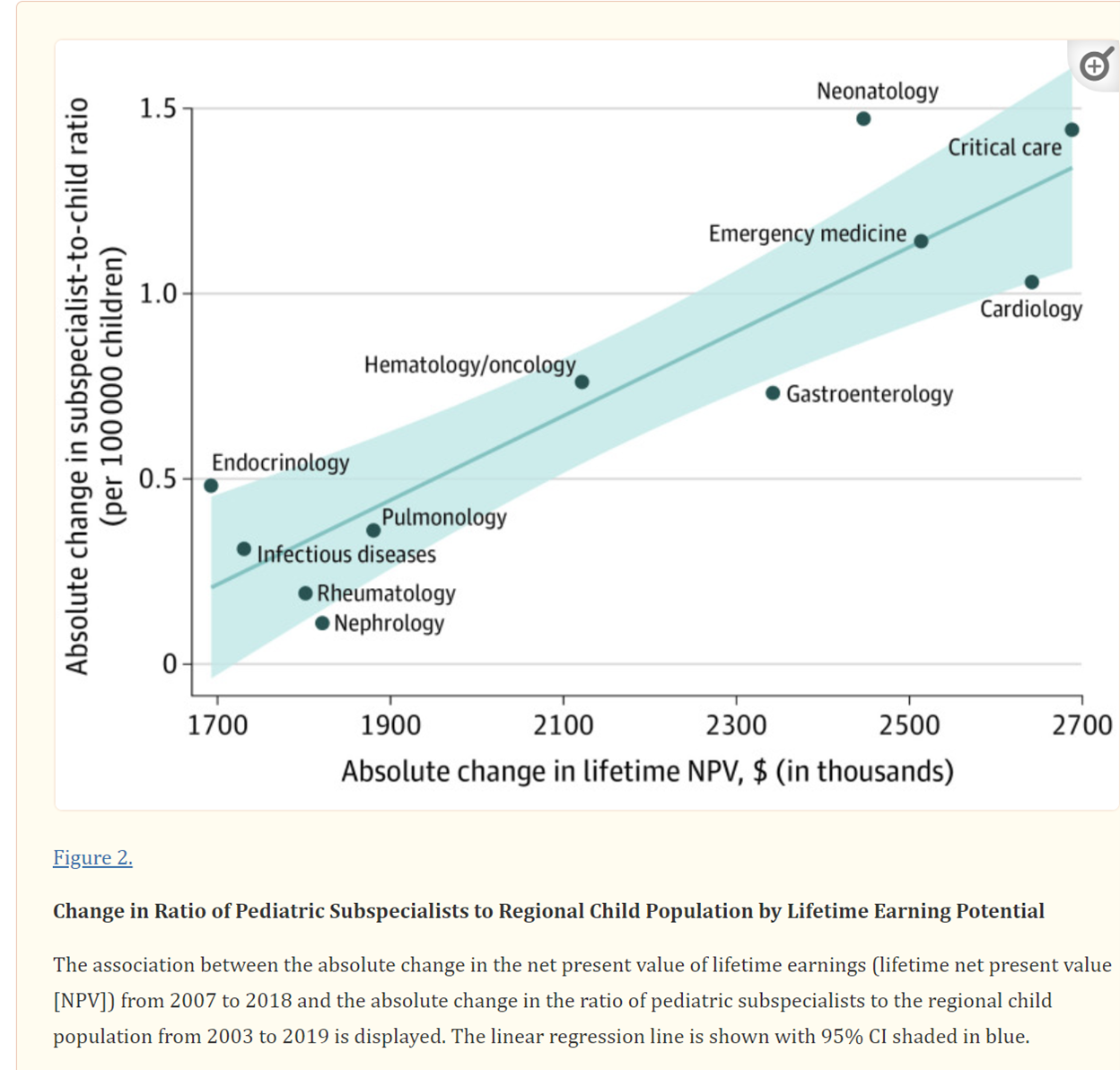
Lifetime earning potential is amongst the most important elements in the decision of medical students and residents in deciding their career choices, and the annual graduate survey conducted by the Pediatric Anesthesiology Program Directors’ Association confirms that it’s also true among our fellows. But don’t judge them too harshly – many of these trainees are completely underwater, drowned by debt due to the high costs of graduate (college + medical school) education. Over the past 50 years, the American graduate educational-industrial-complex has created and perpetuated this educational debt crisis. In the general pediatric subspecialties, “disparate financial returns of fellowship training and subspecialty of choice may influence pediatric workforce distribution if trainees incorporate the economic effect of selecting pediatric subspecialties with lower lifetime earning potential into their career decisions”.3-5 Thus, pediatric subspecialties like endocrinology, infectious diseases, rheumatology, nephrology, and pulmonology are having trouble attracting trainees, whereas higher paying subspecialties like neonatology, cardiology and critical care medicine are not (figure). Indeed, “pediatric[ian] subspecialists often do not experience financial benefits from additional training because there is often no relative increase in compensation after training compared with that of a general pediatrician. Moreover, the delays in garnering increased compensation after training and in repaying educational debt contribute to the negative career long financial impact of fellowship training. These differences cannot be attributed to the differences between private and academic practices.”3-5 Sound familiar?
Why does this matter? “Lifetime earning potential of a subspecialty is strongly associated with multiple measures of current workforce distribution, including distance to subspecialists, the availability of subspecialists across referral regions, and the ratio of subspecialists to the regional pediatric population.”3-5
As anesthesiologists we make significantly more money than primary care physicians like pediatricians. Indeed, this may be one of the most important driving forces in why medical students decide to go into anesthesiology in the first place. But if money is the driving factor, why bother going into a subspecialty like pediatric anesthesiology where starting salaries may be the same or lower than in a general practice, especially when that subspecialty often requires caring for the most fragile patients? Indeed, there may be a financial disincentive in doing so, particularly when accounting for the lost earnings during training, increased debt-repayment costs as interest accrues, and lost time/income contributed towards retirement savings.
Among pediatrician subspecialists, the rate at which fellowship training spots fills correlates with the lifetime financial returns of that specific subspecialty.1 Perhaps this may be one of the root causes of the many unfilled pediatric anesthesiology fellowship spots. Given the high demand for pediatric anesthesiologists (and critical demand for pediatric cardiac anesthesiologists) with a soon-to-be even lower supply of new graduates, a crisis is looming. We are hopeful that shortages will lead to adjusted/higher salaries and “capitalism will work” by recruiting more residents into the specialties. But in the meantime, investigation is warranted to determine what else we could be doing differently.
Recall that there has been a profound discussion of wellness in anesthesiology. We would like to highlight that, despite the stresses we are all under and the ongoing room for improvement in this area, job satisfaction and wellness are much higher for us and our colleagues than among our adult anesthesiology counterparts. There are also many more factors involved in career decisions for most people, including lifestyle, patient complexity and variety, and academic/scholarly interests. Understanding the impact of these elements may help us gain better insight into the problem of the disappearing pediatric anesthesiology fellow. What we know for sure is that workforce projections are murky at best, and that any prior indication of an oversupply of pediatric anesthesiologists now seems way off.6 Indeed, those former projections may have also contributed to the fall off of applicants into our profession.
It is important to recognize that people have many varying factors that weigh into their decisions to pursue specialties while in medical school. The thrill of the work, the discovery, and the knowledge that what we and our colleagues do can affect and improve the lives of our patients and families is certainly one motivating factor. But we will acknowledge that the personal definition of wealth and success can vary from individual to individual, for reasons that are personal, cultural, or influenced by geography, family needs, or circumstance. Furthermore, the pernicious and corrosive effects of medical (and college) school debt cannot be underestimated in today’s world. In 2022, the median medical school debt is $200,000 which may be doubled in the increasingly common 2 physician households. Borrowers with medical school debt may take 20-25 years to repay federal loans in income-driven repayment (IDR) plans.
What are the options out there to prevent what we see as an oncoming professional catastrophe? Federal loan repayment programs and amnesty are one possibility. Unfortunately, we don’t think this is likely in a non-primary care specialty like anesthesiology. Shortening fellowship (currently at 3 years in Pediatrics) was proposed in the pediatrician articles, but not a feasible option for an already compact one-year fellowship. Should we reexamine how fellows are paid? Should we consider paying them on a different scale, and not PGY-5s? Perhaps they should not be considered trainees at all (in the NIH payscale sense) and we should just pay them as junior faculty apprentices? Interestingly, when I (MY) was an anesthesia resident at the University of Pennsylvania in the 1970s, the Department chair, Dr. Harry Wolman, gave his residents and fellows interest free loans that did not have to be repaid IF they remained on staff at the completion of their training.
Are there other reasons that are hindering residents in anesthesiology from pursuing pediatric anesthesiology as a specialty? Could it be that we don’t get to them early enough in their training to make a meaningful impression? Could it be that the patients we first expose them to are healthy, older, and less challenging, and that early exposure to neonates and complex cardiac, craniofacial and neurosurgical children would convince them that we’re not all “rainbows and puppies” at the children’s hospital? Is there a better, more standardized way to approach their education to share with them the joy and challenge of caring for children? Would it be worthwhile to determine if certain residency programs excel at raising future pediatric anesthesiologists and investigating what makes them successful in doing so? Might we need to consider different care models in order to ensure good care for all children? We think the answer to all of these questions is a resounding “Yes, maybe!” and that further research is needed.
While we may be biased, we do believe that every child undergoing surgery deserves outstanding pediatric anesthesia care, and that in the meantime the most important thing we can do is to continue to role model our outstanding, fun, amazing, and intellectually stimulating careers every day for medical students and residents. We encourage you to do the same every day!
What are your thoughts? Do you have any ideas? We’ll publish your responses in an upcoming Readers Response
References
1. Cladis FP, Lockman JL, Lupa MC, et al. Pediatric Anesthesiology Fellowship Positions: Is There a Mismatch? Anesthesia and analgesia. Dec 2019;129(6):1784-1786. doi:10.1213/ane.0000000000004431
2. Yaster M, Davis PJ, Greeley WJ. The American Pediatric Critical Care Anesthesiologist: An Endangered Species Worth Saving. Anesthesia and analgesia. Feb 2019;128(2):204-206. doi:10.1213/ane.0000000000003934
3. Catenaccio E, Rochlin JM, Simon HK. Association of Lifetime Earning Potential and Workforce Distribution Among Pediatric Subspecialists. JAMA pediatrics. Oct 1 2021;175(10):1053-1059. doi:10.1001/jamapediatrics.2021.1912
4. Rochlin JM, Simon HK. Does Fellowship Pay: What Is the Long-term Financial Impact of Subspecialty Training in Pediatrics? Pediatrics. 2011;127(2):254-260. doi:10.1542/peds.2010-1285
5. Catenaccio E, Rochlin JM, Simon HK. Differences in Lifetime Earning Potential for Pediatric Subspecialists. Pediatrics. 2021;147(4)doi:10.1542/peds.2020-027771
6. Muffly MK, Singleton M, Agarwal R, et al. The Pediatric Anesthesiology Workforce: Projecting Supply and Trends 2015-2035. Anesthesia and analgesia. Feb 2018;126(2):568-578. doi:10.1213/ane.0000000000002535
Excellent discussion and warning. I have not looked at anesthesiology salaries in more than 5 years, but when I was the Chief in Seattle, fellowship trained faculty had a slightly higher starting salary. If that is now not the case, our systems have failed in my humble opinion! I also used the career earnings potential as a rational reason for doing a second fellowship year focus on academic training. I was able to get promoted at 5 years for both associate and full professor principally because I was a successful scholar after this advanced training. Fellows better prepared to succeed academically in our department have frequent been promoted to associate and full professor years earlier than their colleagues without this training. Leaders of the system need to make sure we are not causing the extinction of our own specialty!
I talk to many residents who seem disinclined to do fellowship training given the current robust job market. My council is always to take a long view of a career. Medicine in the US is highly politicized with the growth of competition for our jobs by CRNAs increasingly likely. Job security in the future will be driven by the added value we provide by virtue of our training. My first advice to them is to take the extra year and do a fellowship now. That investment in time will likely pay dividends many times over throughout a lifetime career. Which fellowship is the next question and is driven by what someone finds appealing , but they don't often appreciate the many nuanced advantages of practicing pediatric anesthesia. Having transitioned mid-career after 17 years of adult practice, I appreciate the differences that make the everyday work taking care of kids rewarding. I find the collegial culture in a pediatric perioperative environment to be much more enjoyable than in adult practice. It is just harder to be abrasive and unpleasant around kids. In pediatric anesthesia, we enjoy the challenge of practicing in all subspecialty areas - there is less siloed practice than in many adult settings. Helping parents feel comfortable as you take their children from them has rewards. There is also the advantage of lifting small patients and saving your back! Helping trainees understand the value of a fellowship in the context of a career and demonstrating the benefits of pediatric anesthesia practice will hopefully help to meet the looming shortages.