


Patent Ductus Arteriosus in Preterm Infants
Myron Yaster MD, Jim Dinardo MD, Susan Nicolson MD, Lindsey Baptist MD, Viviane Nasr MD MPH

“Despite extensive research in basic science and in clinical settings with thousands of infants over decades, uncertainty and controversy persist regarding the significance, assessment, and management of the patent ductus arteriosus (PDA) in preterm infants, resulting in substantial variability in clinical approach.”1 In today’s PAAD, Ambalavanan et al. review the available evidence to guide evaluation and treatment of preterm infants with prolonged ductal patency. I was actually surprised by many of the findings in this report, particularly in the management of hemodynamically significant PDA (hsPDA), and thought many of you would be as well. I’ve asked our cardiac team to join me in reviewing this article. Myron Yaster MD
Original article
Ambalavanan N, Aucott SW, Salavitabar A, Levy VY; Committee on Fetus and Newborn; Section on Cardiology and Cardiac Surgery. Patent Ductus Arteriosus in Preterm Infants. Pediatrics. 2025 Apr 28:e2025071425. doi: 10.1542/peds.2025-071425. Epub ahead of print. PMID: 40288780.
“In term infants, the ductus arteriosus normally constricts after birth and becomes functionally closed in 90% by 48 hours of age, in nearly all by 96 hours of age, and further delayed in preterm infants. More immature infants have a more pronounced delay, with the ductus remaining open at 4 days of age in approximately 10% of infants born at 30 through 37 weeks’ gestation, 80% of those born at 25 through 28 weeks’ gestation, and >90% of those born at 24 weeks’ gestation. By day 7 after birth, those rates decline to approximately 2%, 65%, and 87%, respectively.”1 Even in premature infants with respiratory distress syndrome, the vast majority will have spontaneous closure of their PDA. Because of this, “prophylactic medical interventions (those not guided by knowledge of PDA status) are not recommended at any age or birth weight for the purpose of reducing the risk of a symptomatic PDA, as there are no effects on mortality, BPD, or neurodevelopmental impairment.”1
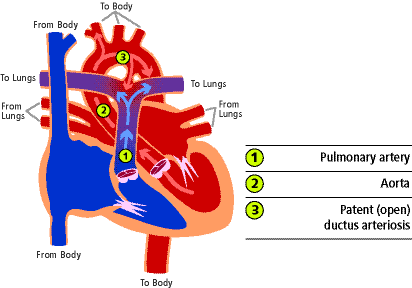
“While the ductus remains open, blood typically flows left-to-right from the aorta into the pulmonary arteries. As pulmonary vascular resistance declines in the initial days after birth, there is an augmented diversion of aortic blood flow into the pulmonary circulation, known as the “ductal steal.” This phenomenon results in additional blood flow through the lungs, predisposing to the development of pulmonary congestion, pulmonary edema, and exacerbated respiratory failure. Other adverse effects include prolonged assisted ventilation and higher rates of death, bronchopulmonary dysplasia (BPD), pulmonary hemorrhage, necrotizing enterocolitis (NEC), impaired renal function, intraventricular hemorrhage (IVH), periventricular leukomalacia (PVL), and cerebral palsy (CP).”1
“Neonatal echocardiography has a critical role for PDA diagnosis and evaluation of therapeutic responses.2,2b Defining an hsPDA involves careful determination of: (1) PDA shunt assessment and its impact on the systemic and pulmonary circulations; (2) myocardial and mitral valve function evaluation, especially in the context of the potential for myocardial ischemia secondary to impaired coronary artery perfusion; and (3) clinically relevant characteristics that modify the effects a shunt may have to an already compromised milieu.1 (figure)

Prostaglandin inhibitor drugs (indomethacin, ibuprofen, and acetaminophen) are very effective in symptomatic PDA closure compared with no therapy. The use of NSAIDs, particularly indomethacin, to pharmacologically close a PDA has been well established since the 1970s.3 I (MY) must admit that I was shocked to learn that acetaminiophen, which is thought to act more centrally, was also effective, although perhaps not as effective as ibuprofen.4,5 In most PDA cases, watchful waiting is now the norm. In hsPDA, for many decades when medical management fails or is too dangerous, “surgical closure of the PDA is accomplished very predictably either by a clip application or by ligation. Surgical closure has low morbidity and mortality even in very preterm infants.”1 “Infants who undergo surgical ligation have been found to be more likely to develop BPD,ROP, and neurodevelopmental impairment. Because of these risks and the risks of anesthesia and transfer from the NICU to the operating room, surgical closure is often reserved for infants who have a persistent PDA despite medical therapy (usually after 2 or more failed courses) or in whom medical therapy is contraindicated.”1
Transcatheter closure of a PDA has become increasingly common.6 “Transcatheter closure has classically been the procedure of choice for definitive PDA occlusion in adults, children, and infants weighing >6 kg and has become a first-line intervention for much smaller patients in many institutions as devices and techniques have improved and developed.”1 “The Amplatzer Piccolo Occluder received FDA approval in 2019 and became the first device approved for PDA closure in patients weighing ≥700 g.7”1 It is effective in >95% of patients.
The challenges to using transcatheter or surgical closure strategies are establishing the appropriate timing, the selection of patients, and the experience and expertise within each center. Transcatheter closure occurs either in the cath lab or at the bedside in the NICU using echocardiographic guidance. Although the article does not discuss the need for anesthesia, in our experience, cath lab closures are performed under general anesthesia and NICU, echo guided closures are not. For many of these infants, respiratory failure is severe enough to require mechanical ventilation at relatively high driving pressure, rate, and PEEP. In the most extreme instances HFJV or HFOV is necessary to reduce the risk of mechanical lung injury and facilitate adequate ventilation and oxygenation.
Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Ambalavanan N, Aucott SW, Salavitabar A, Levy VY. Patent Ductus Arteriosus in Preterm Infants. Pediatrics 2025 (In eng). DOI: 10.1542/peds.2025-071425.
2. Shepherd JL, Noori S. What is a hemodynamically significant PDA in preterm infants? Congenit Heart Dis 2019;14(1):21–26. (In eng). DOI: 10.1111/chd.12727.
2b. Zhang, K., Ray, A. M. & DiNardo, J. A. Optimizing Hemodynamic Management in the Neonatal Intensive Care Unit: Leveraging Neonatal Echocardiography. J. Cardiothorac. Vasc. Anesthesia 38, 1630–1633 (2024).
3. Heymann MA, Rudolph AM, Silverman NH. Closure of the ductus arteriosus in premature infants by inhibition of prostaglandin synthesis. NEnglJMed 1976;295(10):530–533.
4. Jasani B, Mitra S, Shah PS. Paracetamol (acetaminophen) for patent ductus arteriosus in preterm or low birth weight infants. The Cochrane database of systematic reviews 2022;12:Cd010061. (In eng). DOI: 10.1002/14651858.CD010061.pub5.
5. Mitra S, Florez ID, Tamayo ME, et al. Association of Placebo, Indomethacin, Ibuprofen, and Acetaminophen With Closure of Hemodynamically Significant Patent Ductus Arteriosus in Preterm Infants: A Systematic Review and Meta-analysis. Jama 2018;319(12):1221–1238. (In eng). DOI: 10.1001/jama.2018.1896.
6. Kuntz MT, Staffa SJ, Graham D, et al. Trend and Outcomes for Surgical Versus Transcatheter Patent Ductus Arteriosus Closure in Neonates and Infants at US Children's Hospitals. J Am Heart Assoc 2022;11(1):e022776. (In eng). DOI: 10.1161/jaha.121.022776.
7. Sathanandam SK, Gutfinger D, O'Brien L, et al. Amplatzer Piccolo Occluder clinical trial for percutaneous closure of the patent ductus arteriosus in patients ≥700 grams. Catheter Cardiovasc Interv 2020;96(6):1266–1276. (In eng). DOI: 10.1002/ccd.28973.