


Partial Heart Transplant in Congenital Cardiac Surgery: One and Done?
Lindsey Loveland, Susan Nicolson, James DiNardo, Viviane Nasr

Original article
Rajab TK, Vogel AD, Turek JW. Partial Heart Transplant in Congenital Cardiac Surgery. JAMA Surg. 2024 Jul 17. doi: 10.1001/jamasurg.2024.1567. Epub ahead of print. PMID: 39018045.
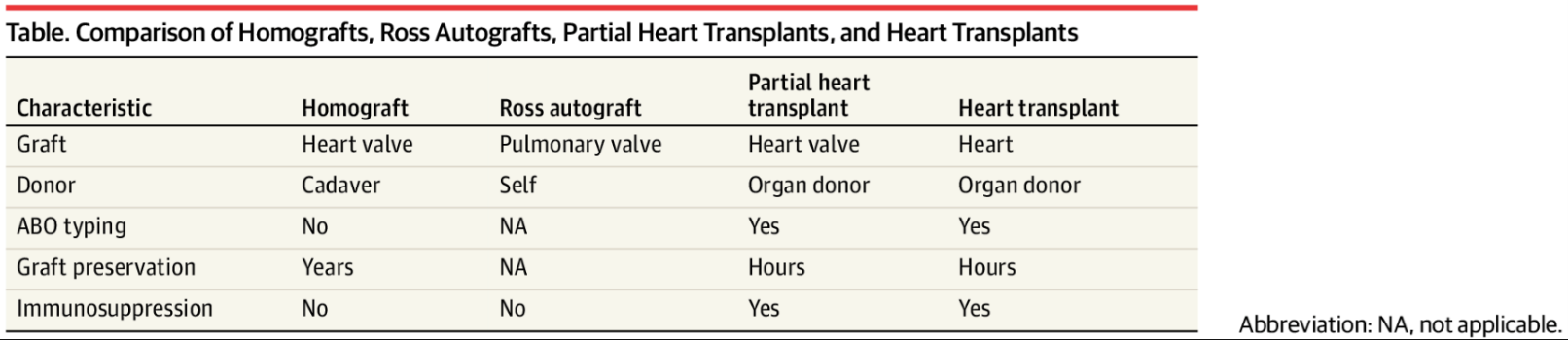
“Partial Heart transplant” is a very catchy title, leading one to be very curious! It might be a little bit misleading in some ways, but truer than you might imagine! The article and problem centers around infants with congenital heart valve issues – for example aortic stenosis that might be treated with a valve implant or a Ross procedure in which the diseased aortic valve is replaced with the patient’s own pulmonary valve followed by replacement of the pulmonary valve with a pulmonary homograft. Homografts are heart valves procured from human cadavers and preserved without maintaining functional valve cells. This traditional approach to treatment of valve disorders in infants and children is problematic because heart valve implants and homografts do not grow and ultimately calcify. These infants and children are committed to multiple re-operations to either upsize until they can have an adult sized implant or to replace a dysfunctional valve.
Rajab et al.1 describe “partial heart transplant” meaning implantation of only the part of the heart containing the necessary valve that still contains functional valve cells and is treated like tissue for transplant. These implanted valves are projected to grow, be resistant to wear and tear degradation via self-repair, and resist endocarditis like heart valves contained in transplants. Full heart transplants seldom fail from primary valve dysfunction, so it is not unreasonable to expect a heart valve transplant to last a lifetime.
Valves used in partial heart transplants grow despite immune suppression. We know that Ross pulmonary autografts in children grow despite devascularization and reimplantation. Preliminary data in piglets and humans show that partial heart transplants grow despite immunosuppression, devascularization and reimplantation. The first human partial heart transplant was performed approximately one year ago and shows good adaptive valve growth and function on short term follow up.2
Partial heart transplant – would it be more accurate to call it heart valve transplant? – suffers from a similar barrier that full heart transplant suffers– a centralized system for equitable allocation. Surgeons planning this procedure need to coordinate with individual organ procurement organizations. The challenge of this is exacerbated by the shortage of donor hearts. It is worth noting that partial heart transplant donors are potentially a much larger donor pool than full organ transplant. Ventricular function is not an issue for valve transplants and domino transplants from recipients could also possibly be used as partial heart transplants but not heart transplants.
The recipients of these valves with viable cells do need immunosuppression and all the risks that go with it. So, the risk of serial implants must be greater than the risk of immunosuppression. It is worth noting that stopping immune suppression for a partial heart transplant would simply turn the implant into a non-growing homograft!3 There also is a lack of long-term data. Maybe at a certain age or size children who received these valves can stop their immunosuppression? The technical aspects of “partial heart transplant” resemble homograft valve replacement from a surgeon’s perspective and heart transplant from a medical perspective. While details of the long-term follow-up would certainly need to be sorted out, congenital cardiac surgical centers have all the necessary tools and teams to perform these procedures. The team and institution that reported this partial heart transplant is working to create a central system for organ allocation and intends to include other stake holders soon.
There are certainly many more questions, but it seems this is a solution that gets around some of the significant limitations of valve replacement surgery in smaller than adult size children?
Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Rajab TK, Vogel AD, Turek JW. Partial Heart Transplant in Congenital Cardiac Surgery. JAMA surgery 2024 (In eng). DOI: 10.1001/jamasurg.2024.1567.
2. Turek JW, Kang L, Overbey DM, Carboni MP, Rajab TK. Partial Heart Transplant in a Neonate With Irreparable Truncal Valve Dysfunction. Jama 2024;331(1):60-64. (In eng). DOI: 10.1001/jama.2023.23823.
3. Mehrotra R, Srivastava S, Airan B, et al. Aortic valve replacement with a homovital valve. Tex Heart Inst J 1997;24(3):221-2. (In eng).