


Mitigating the systemic loss of nitrous oxide: a narrative review and data-driven practice analysis
Germana Silva MD, Diane Wood Gordon MD

Regular readers of the PAAD know that the Society for Pediatric Anesthesia (from the website) has a “Special Interest Group for Sustainability” that brings together pediatric anesthesiologists with a passion for learning, teaching, and practicing ways to reduce the environmental impact of anesthesia and the wider operating room environment. The SIG facilitates education on sustainability topics at meetings, fosters collaboration across institutions, promotes sharing of ideas for projects and publications, and maintains the creative energy of pediatric anesthesiologists working for changes in their hospitals. Further, the Sustainability SIG is helping to recruit pediatric anesthesia groups to a multi-institutional quality improvement and implementation science project to reduce GHG emissions! Visit the website to learn more Project Spruce (Saving our Planet by RedUcing Carbon Emissions)”. We’ve posted several PAADs on Project Spruce, including a review of the article by Hansen et al.1 (06/27/2023 https://ronlitman.substack.com/p/more-on-project-spruce-saving-our) who over a five year period were able to reduce measured green house gas (GHG) emissions from inhaled anesthetic agents by 86%. One of the most surprising findings to almost all of us was that a large amount of nitrous oxide waste came from “significant leaks that occur from central supply nitrous oxide tanks.”1
When I taught students in the operating rooms, I would always quiz them on how much oxygen was in the transport E cylinder and how long would it last. Because it exists only in a gas state, a full tank of oxygen had about 660 Liters of oxygen (at 2,200 PSI). I would do the same for the E cylinders of nitrous oxide, particularly while I supervised their anesthesia machine checkout. Of course, this was a bit of a trick question because in the E cylinder, nitrous oxide exists as a liquid, so how much nitrous was in the tank was unknown until the pressure starts to fall below 750 when the liquid is exhausted. (A brand new tank of nitrous has about 1,600 L, much of which is in liquid form). In today’s PAAD, Chesebro and Gandhi2 take another look at losses from central N2O supply systems and how you can spearhead facility-level engagement, action and change.
And to help facilitate your understanding of the various nitrous storage vessels, Dr. Gordon, who reviews sustainability articles for the PAAD, took some pictures which are worth a thousand words! Myron Yaster MD
Original article
Chesebro BB, Gandhi S. Mitigating the systemic loss of nitrous oxide: a narrative review and data-driven practice analysis. Br J Anaesth. 2024 Dec;133(6):1413-1418. doi: 10.1016/j.bja.2024.08.028. Epub 2024 Sep 24. PMID: 39322471.
Background
All of you are familiar with the E cylinders attached to your anesthesia machines which serve as either the primary source of oxygen and nitrous oxide for your anesthetics or as backups to wall pipeline supplies if they fail. Have you ever wondered where the wall supplies come from and how much nitrous oxide are in the various size cylinders? I (DWG) took some pictures of N2O storage vessels to help.

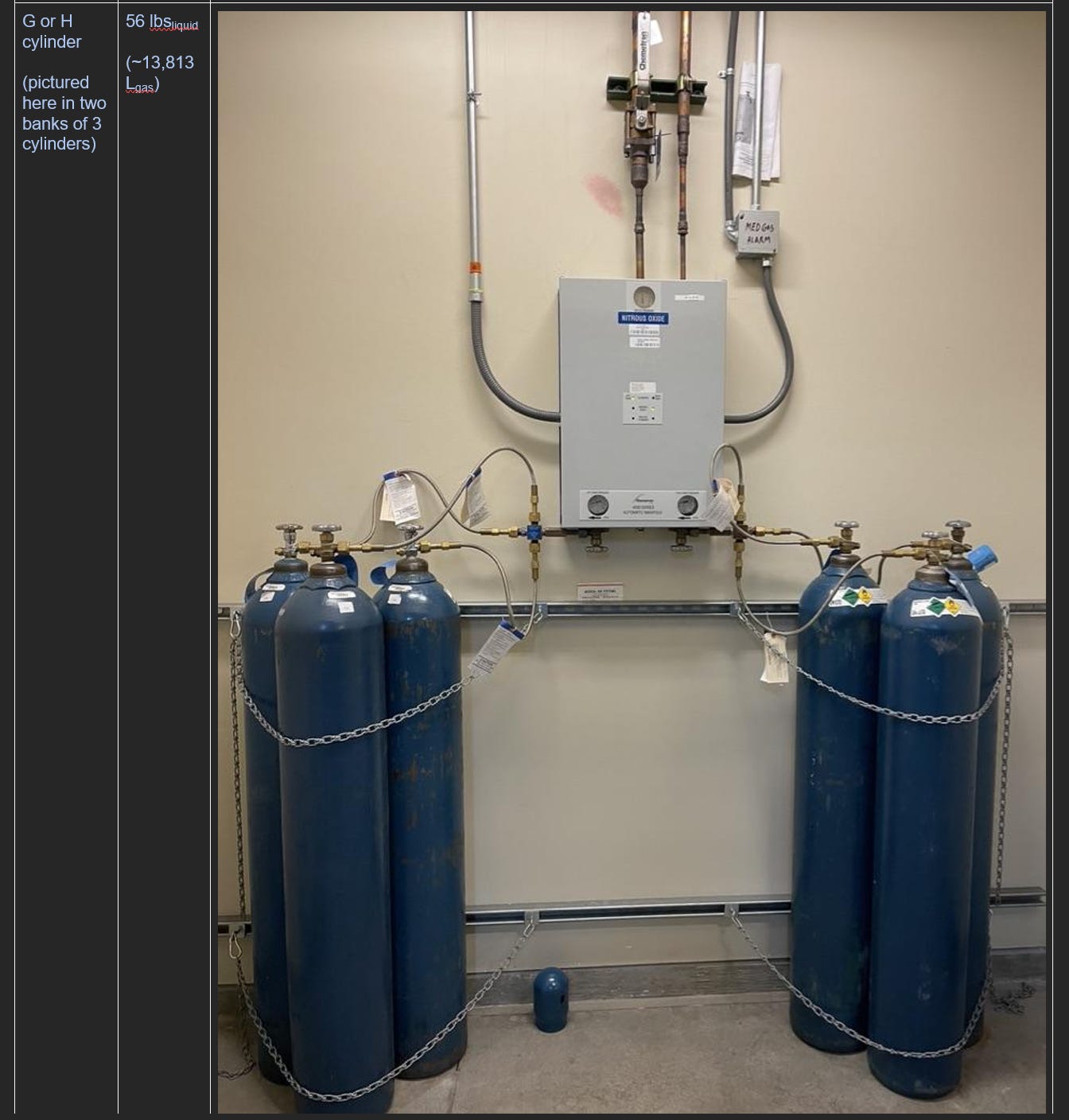

Nitrous Oxide (N2O) has a long atmospheric lifetime, a high global warming potential and is the most prevalent ozone-depleting substance on earth. Nitrous Oxide accounts for 84-94% of anesthesia-related greenhouse gas emissions in Ireland, Austria, and the NHS system of the UK. Hospital N2O is supplied through a central pipeline system that uses large-volume tanks (H-cylinders) or cryogenic tanks (dewars) as the reservoir. This central system is connected to a pressure-regulating manifold and then to long pipes that end in wall outlets in each clinical use location. Discrepancies in the volume of clinically-administered N2O compared to volumes of purchased N2O have previously been reported in Australia3 and the UK.4-6
Ok, so what did they find?
The authors compared clinical usage of N2O to the purchased volume of N2O at 47 hospitals (mix of private and academic, 1 is a freestanding pediatric hospital and 6 others are tertiary hospitals that do pediatric anesthesia*) in the US., median N2O waste was 93% (range 47.2-99.8%). Leaks were found in all hospitals and did not correlate with hospital size (Figure 1). Most hospitals in this cohort used H-cylinders as the source of central N2O, but several used cryogenic tanks, and the leak was large with both sources of central N2O*. *This information is from personal communication with the author but wasn’t included in the manuscript.

Impact of Transitioning to Portable E-cylinders
Transitioning to portable (E-cylinders) of N2O at one large hospital resulted in a 97.6% reduction in N2O “utilization” (defined as N2O leaving its container- either for patient use or due to leakage). After deactivating the central nitrous system, the amount of N2O purchased nearly matched the clinical use of N2O, reinforcing the finding that a significant amount of N2O was previously leaking (Figure 2). Across 47 hospitals and 834 clinical locations, the projected median number of days between E-cylinder exchanges (exchange frequency) per individual location is 414 days (range 16–5497 days). After 12 months of using portable N2O systems in seven facilities, the actual exchange frequencies closely aligned with these projections, confirming the accuracy of the estimated needs.

In every hospital, very large reductions in greenhouse gas emissions resulted from deactivating the central N2O pipeline. Other benefits include reduced occupational exposure, lower cost and time burden from maintaining the central pipeline, and faster detection of leaks due to the independent source of N2O for individual anesthesia machines. Finally, not installing central N2O in hospitals that are being built saves considerable capital.
The Role of Anesthesiologists
“As the primary end-users of N2O, anesthesia clinicians are in an ideal position to lay the initial groundwork by guiding an institution-specific assessment of N2O practices.” N2O usage per anesthesia location is a helpful metric for predicting the rate of E-cylinder exchanges that will be required once the transition away from the central N2O pipeline is accomplished.
PAAD author notes:
DG- reduced clinical usage prior to disconnecting from the central pipeline will reduce the rate of E-cylinder exchanges required but it isn’t a prerequisite for making this transition. The knee-jerk reaction of most hospitals to the reality of rampant leaks in the central N2O system will be “that can’t be true at OUR hospital”. Chesebro’s paper adds to the growing body of literature proving that leaks from central nitrous oxide systems are, in fact, ubiquitous. Proof of the leak at your hospital shouldn’t be necessary, but data always makes a better argument. Procurement data for N2O is easy to acquire (follow the money!) and clinical usage data can be pulled from electronic medical records through aftermarket software or tools built-in to the EMR.
GS- The transition to portable N2O systems is not just an environmental necessity—it is an opportunity for leadership in the healthcare sector. It is a call to action for anesthesiologists to engage in multidisciplinary efforts to address climate change, reduce waste, and improve safety in the perioperative setting.
Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Hansen EE, Chiem JL, Righter-Foss K, et al. Project SPRUCE: Saving Our Planet by Reducing Carbon Emissions, a Pediatric Anesthesia Sustainability Quality Improvement Initiative. Anesthesia and analgesia 2023;137(1):98-107. (In eng). DOI: 10.1213/ane.0000000000006421.
2. Chesebro BB, Gandhi S. Mitigating the systemic loss of nitrous oxide: a narrative review and data-driven practice analysis. British journal of anaesthesia 2024;133(6):1413-1418. (In eng). DOI: 10.1016/j.bja.2024.08.028.
3. Seglenieks R, Wong A, Pearson F, McGain F. Discrepancy between procurement and clinical use of nitrous oxide: waste not, want not. British journal of anaesthesia 2022;128(1):e32-e34. (In eng). DOI: 10.1016/j.bja.2021.10.021.
4. Chakera A. Driving down embedded emissions from medical nitrous oxide. BMJ (Clinical research ed) 2021;375:n2922. (In eng). DOI: 10.1136/bmj.n2922.
5. Chakera A, Harrison S, Mitchell J, Oliver C, Ralph M, Shelton C. The Nitrous Oxide Project: assessment of advocacy and national directives to deliver mitigation of anaesthetic nitrous oxide. Anaesthesia 2024;79(3):270-277. (In eng). DOI: 10.1111/anae.16211.
6. Southall P, Shelton C, Chakera A. Consensus on decommissioning piped nitrous oxide from UK and Ireland operating theatre suites: a rational approach to an increasingly ignoble gas. Anaesthesia 2024;79(12):1274-1279. (In eng). DOI: 10.1111/anae.16407.