
Medication error
Myron Yaster MD and Jayant K. Deshpande MD MPH

In a previous PAAD (Nov 9,2022: “Trust but verify”), we discussed medication errors in anesthesiology. I received today’s article(1) from one of our readers, Dr. Scott Hines, a pediatric anesthesiologist at Children's Hospital of the King's Daughters. Scott trained at CHOP and was a colleague of the late Dr. Ron Litman who was a strong advocate for improving drug administration safety. Although I do my best to scan as much of the literature as I can, if you find something that you think is PAAD worthy just let me know and I’ll try to have our team review it. Myron Yaster MD
Original article
Institute for Safe Medication Practices: Obstetrical Patient Receives Ampule of Digoxin Instead of BUPivacaine for Spinal Anesthesia. https://www.ismp.org/resources/obstetrical-patient-receives-ampule-digoxin-instead-bupivacaine-spinal-anesthesia
A fundamental difference in how we practice medicine as anesthesiologists as compared to the rest of medicine involves drug administration. We “order” the drugs the patient needs, draw up (“dispense”) our own drugs, administer them to patients without any oversight, and personally document what we’ve administered in the anesthetic record. And we do this in a working environment that is distracting, and we rely on “on situational awareness, mental focus, and vigilance in order to reduce the chance of medication errors (MEs) occurring. However, human errors are an inevitable outcome of poor human reliability; so it is essential that steps are taken to minimize errors and harm”.(2) Think about the chain of events that occur in how other specialties in your hospital do this: 1) a doctor or increasingly a nurse practitioner or physician’s assistant makes a diagnosis and enters an order for a drug on the EMR, 2) the order is transmitted to a pharmacy whereupon a pharmacist checks the dose and the drug, draws up the drug and labels it, sends it to the floor, 3) there a nurse checks the order against what was ordered and what was actually sent from the pharmacy to the floor; if the drug is a “high risk” medication or is being given via an infusion pump, the nurse finds another nurse to double check the drug and pump programming (“independent double verification”) , and 4) then documents in the EMR.
Our anesthesia process is core to how we practice, but does it meet the current safety standards? Indeed, others in the hospital, particularly those tasked with quality and safety, think that how we administer drugs is unsafe, antediluvian, and well nuts. In today’s PAAD, a pregnant patient undergoing a C section was accidentally given digoxin rather than bupivacaine for her spinal anesthetic. “Ouch!”
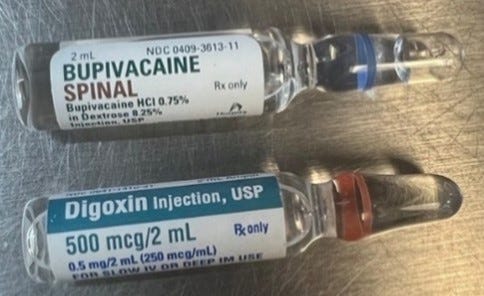
That this happened shouldn’t be at all surprising. Both ampules look alike (figure). One recent, single institution review “analyzed inadvertent neuraxial cardiovascular medication administration errors reported between 1972 and 2022. Among the 33 events reported, digoxin was the medication most commonly administered in error and was associated with paraplegia and encephalopathy in eight patients.”(3)
What can be done to prevent this type of error? A 2nd person verification check is often recommended particularly when high risk medications like insulin, heparin and protamine are given. We think it may be impractical for more commonly used medications like spinal bupivacaine. An alternative may be technologic using automated labeling systems with bar codes and oral read aloud feedback(4) and a medication cart template to organize how drugs were laid out in your work area.(5) Having the US FDA demand how drugs are packaged and labeled to prevent the kind of confusion that occurs with look-a-likes like spinal bupivacaine and digoxin would be great but doesn’t appear to be likely in the near future. Although the authors of the ISMP article point the finger at ampules we think that this type of error is just as easily or even more easily made with vials because the print is so small.
The ISMP article is short and well worth the few minutes it takes to read it. We recommend that you do so and share it with your colleagues. What are you doing in your practice to minimize medication errors? Send us your thoughts and we’ll publish in a Friday reader response.
References
1. Institute for Safe Medication Practices (ISMP). Obstetrical patient receives ampule of digoxin instead of bupivacaine for spinal anesthesia, 2023.
2. Mackay E, Jennings J, Webber S. Medicines safety in anaesthetic practice. BJA Educ 2019;19:151-7.
3. Patel S. Cardiovascular Drug Administration Errors During Neuraxial Anesthesia or Analgesia-A Narrative Review. J Cardiothorac Vasc Anesth 2023;37:291-8.
4. Thomas JJ, Bashqoy F, Brinton JT, Guffey P, Yaster M. Integration of the Codonics Safe Label System(®) and the Omnicell XT(®) Anesthesia Workstation into Pediatric Anesthesia Practice: Utilizing Technology to Increase Medication Labeling Compliance and Decrease Medication Discrepancies While Maintaining User Acceptability. Hosp Pharm 2022;57:11-6.
5. Grigg EB, Martin LD, Ross FJ, Roesler A, Rampersad SE, Haberkern C, Low DKW, Carlin K, Martin LD. Assessing the Impact of the Anesthesia Medication Template on Medication Errors During Anesthesia: A Prospective Study. Anesth Analg 2017;124:1617-25.