
In Search of Quality Metrics Specific Solely To Congenital Cardiac Anesthesia
Susan Nicolson, Lindsey Loveland, James DiNardo, Viviane Nasr

Original article
Brown ML, Dorste A, Adams PS, Caplan LA, Gleich SJ, Hernandez JL, Riegger LQ; Quality and Safety Committee of the Congenital Cardiac Anesthesia Society. Proposed Quality Metrics for Congenital Cardiac Anesthesia: A Scoping Review. Anesth Analg. 2024 Oct 15. doi: 10.1213/ANE.0000000000007208. Epub ahead of print. PMID: 39405258.
Congenital cardiac anesthesiologists care for high-risk patients undergoing high -risk procedures with the potential for significant peri-operative morbidity and mortality. Quality metrics are quantifiable measures used to assess the clinical performance, care quality and safety measures of health care providers and organizations. Metrics need to address meaningful, patient-centered outcomes with evidence to support them, using quantitative measurements and estimates of anticipated benefits and harm. Congenital cardiac anesthesiology has lagged congenital cardiology and cardiac surgery in identifying quality metrics for the specialty.
In 2020 the Congenital Cardiac Anesthesia Society inaugurated a Quality and Safety Committee. One of the committee’s first tasks was to undertake a scoping review of quality metrics for congenital cardiac anesthesia.1 A scoping review is a type of evidence synthesis that systematically identifies and maps the available evidence on a topic, concept or issue with the aim of informing practice and providing direction for data collection and future research priorities. There are 5 stages of a scoping review: 1. identify the question, 2. identify relevant studies, 3. study selection, 4. map out the data, 5. summarize, synthetize and report the results. The committee identified 31 candidate metrics which were stratified using the Donabedian model that uses 3 categories to evaluate the quality of health care: structure, process and outcomes.2
Initially 3649 studies published between 2010 and 2021 were identified, 157 duplicates were removed. An additional 3340 studies were removed after abstract review leaving 137 articles that underwent full review. Only 30 articles were identified with quality metrics or data related to quality for congenital cardiac anesthesia. These articles became the basis for assessment of existing data to validate quality metrics for the specialty. Each of the 30 articles were read and reviewed by 6 of the paper’s authors.3 Each reviewer voted on whether to include each metric as a proposed quality metric based on the supporting literature and relationship to the scope of the current practice. The reviewers decided to include only metrics that were unanimously supported (6 of 6 votes). Only 5 candidate metrics for tracking quality in congenital cardiac anesthesia met these criteria. (see Table I).
Table I Quality Metrics (category) For Congenital Cardiac Anesthesia with Proposed Definitions
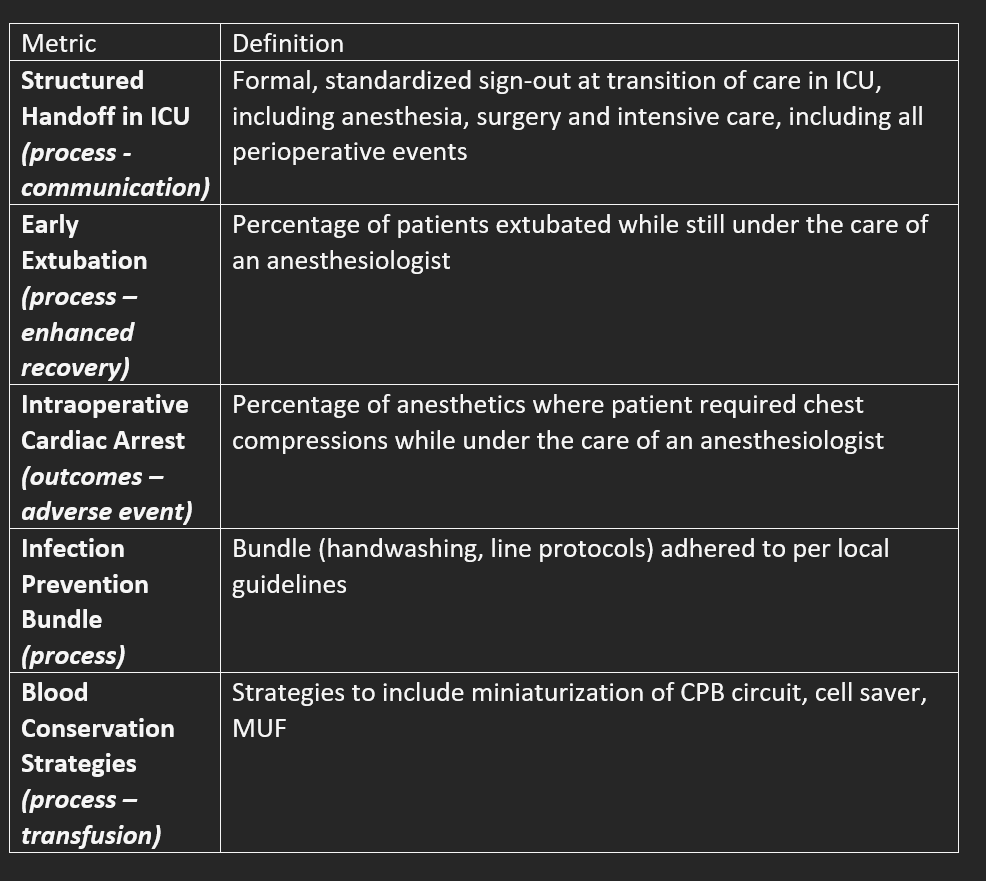
There were additional metrics that did not reach consensus but did a achieve support by 5 of the 6 reviewers: regularly scheduled QI/safety conferences, reintubation rate within 2 hours after extubation by an anesthesiologist, appropriate antibiotic choice and time of administration, availability of point of care testing, near-infrared spectroscopy, and ultrasound for placement of arterial and venous lines.
Outcomes in congenital cardiac anesthesia are complex and dependent of many factors, some patient specific, some specific to the procedure itself, and some an interaction of multiple perioperative factors. Although congenital cardiac anesthesia is a critical component of outcome, it has been difficult to identify metrics specific solely to anesthesia. The authors have shown that there is limited quality data in the literature and emphasize the need for more primary research on quality metrics for the specialty.
Data collection of the 5 quality metrics proposed by Brown et al., once there is agreement on the metrics and consensus on the definitions, will enable a comparison of management and outcomes among practitioners and institutions and creation of benchmarks.
Send your thoughts and comments to Myron who will post in a Friday reader response
References
1. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC medical research methodology 2018;18(1):143. (In eng). DOI: 10.1186/s12874-018-0611-x.
2. Donabedian A. Evaluating the quality of medical care. 1966. Milbank Q 2005;83(4):691-729. (In eng). DOI: 10.1111/j.1468-0009.2005.00397.x.
3. Brown ML, Dorste A, Adams PS, et al. Proposed Quality Metrics for Congenital Cardiac Anesthesia: A Scoping Review. Anesthesia and analgesia 2024 (In eng). DOI: 10.1213/ane.0000000000007208.