



An urban legend: An elderly man comes to the Johns Hopkins Hospital emergency department with a chief complaint of “difficulty walking”. He is sent on a gurney to the MRI suite for diagnostic imaging. On arrival and transfer to the MRI table it’s noted that he is missing his prosthetic limb.
OK, you get the point, the art of taking a proper history and physical examination has inexorably been lost. We compensate for this with an increasing use of laboratory tests and diagnostic imaging studies. Indeed, I’ve wondered for a very long time if a great proportion of the MRIs for which we provide anesthesia is simply unnecessary and out of control…just think of the enormous number of MRIs for autism or for premie graduate follow up. Aside from anesthetic risks (almost universally down played) the MRI environment is very dangerous and potentially lethal. Today’s PAAD discusses how the use of a simple time out and checklist protocol and human behavioral and social factors were used to improve compliance in a quality improvement protocol. Myron Yaster MD
But first a word from Dr. Glaucomflecken
Original article
Joselyn AS, Teddy DA, Jose R, Shanthini S, Joseph L, Rai E, Williams A. Improving safety in anesthetized patients undergoing magnetic resonance imaging-Concept of time-out in the MRI suite and measures to improve adherence to time-out protocol. Paediatr Anaesth. 2023 May;33(5):370-376. PMID: 36620011
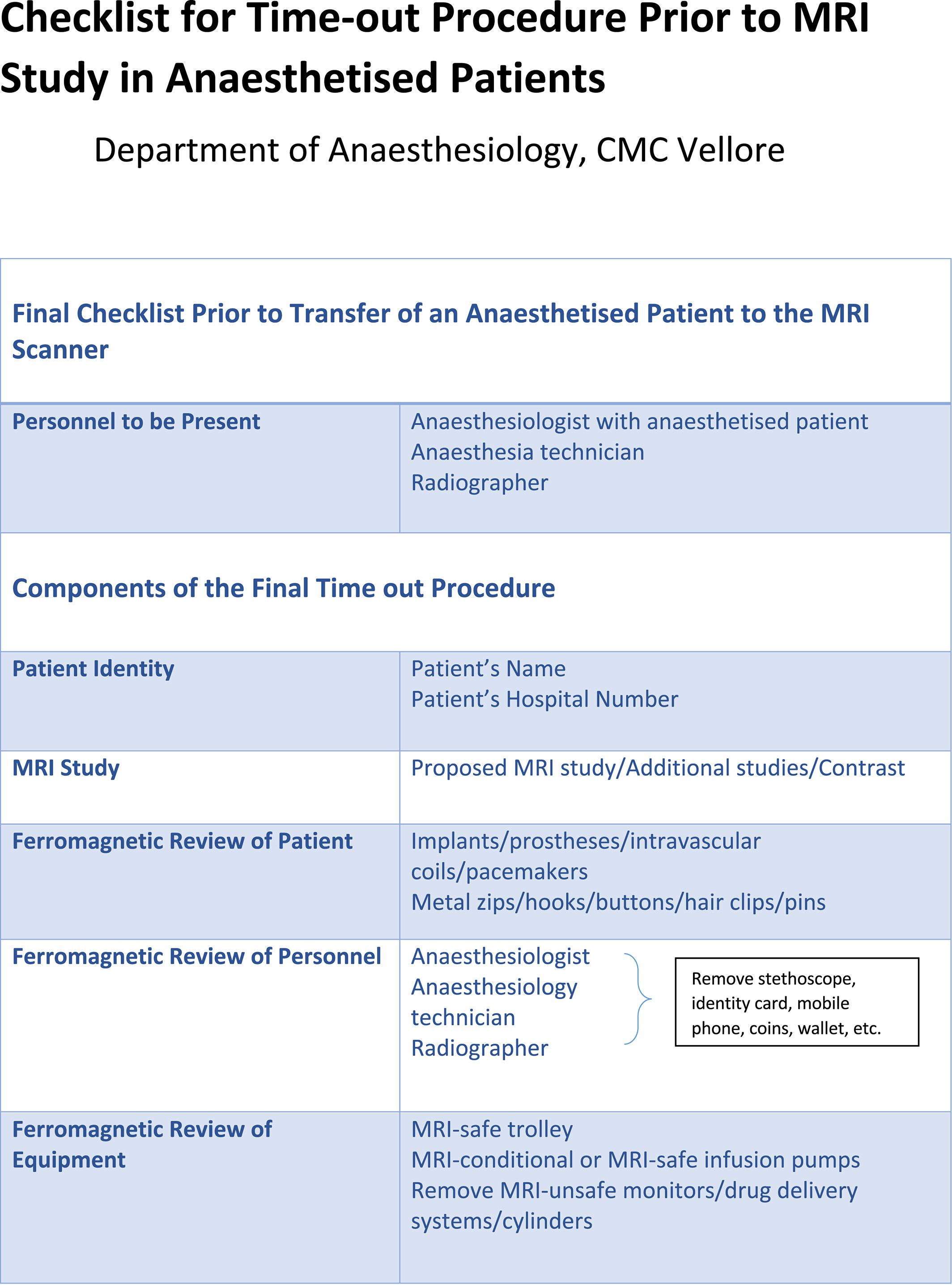
Fundamentally, how can we prevent lethal accidents in MRI zone 4 and protect ourselves and our patients from ferromagnetic projectile injury inside an MRI? Training of personnel using Powerpoint lectures/modules and testing, albeit important, simply doesn’t cut it. After several near misses, Joseyln et al.1, instituted a time out by radiographers and anesthesiologists using a formal checklist for all equipment and personnel before entering the MRI (figure) to prevent these potentially lethal accidents. The checklists were well designed and the product of work by both radiologists and anesthesiologists. Sounds pretty simple doesn’t it? Unfortunately, implementation of the new protocol wasn’t so easy and after its introduction, the compliance rate was only 13%. Sounds familiar doesn’t it? The authors blamed “post graduates and junior medical officers”. We suspect that everyone involved including senior staff were equally responsible. Indeed, any change in how we work, like washing your hands, how you wash your hands, prepping for central line insertion to name a few are often met with similar challenges.
Today’s PAAD 1 employed a quality improvement initiative utilizing the model for improvement initiated by the Institute of Healthcare Improvement.2, 3 The tests of change to improve compliance to time-out protocol were performed through a PDSA (Plan-Do-Study-Act) cycle. Compliance increased to 86% and now approaches 100%.
Needless to say, anesthesia personnel should perform the usual pre-anesthetic checklist encompassing patient identification, procedure confirmation, allergies, and important medical information prior to induction and prior to the subsequent MRI safety checklist to be performed prior to entering MRI zone 4.
How do you deal with this in your practice? Have you had near misses? Do you have a checklist similar to the one used in the article? Do you have an ferromagnetic detector/alarm system in place at the entrance to the MRI? Are personnel wanded? Are lockers/cubbyholes provided for storage of MRI unsafe personal items? Are underwire bras forbidden? (as they were at CHOP) Send Myron your thoughts and we’ll post in the Friday reader response.
References
1. Joselyn AS, Teddy DA, Jose R, et al. Improving safety in anesthetized patients undergoing magnetic resonance imaging-Concept of time-out in the MRI suite and measures to improve adherence to time-out protocol. Paediatric anaesthesia. May 2023;33(5):370-376. doi:10.1111/pan.14627
2. Jones B, Vaux E, Olsson-Brown A. How to get started in quality improvement. BMJ (Clinical research ed). 2019;364
3. Berman L, Raval MV, Goldin A. Process improvement strategies: Designing and implementing quality improvement research. Elsevier; 2018:379-385.