
How low is too low? On those “soft” blood pressures under anesthesia.
Ethan Sanford MD and Justin L. Lockman MD MSEd

phenylephrine to treat hypotension. As the attending, after turning the anesthetic back on, you calmly (or as calmly as you can) explain that normal blood pressures are lower in children and neonates and we permissively allow lower blood pressures in these patients without compromising patient outcomes. But how low is too low, and when should we intervene?
“In November 2022, the Anesthesia Patient Safety Foundation held a Consensus Conference on Hemodynamic Instability with invited experts. The objective was to review the science and use expert consensus to produce best practice recommendations to address the issue of perioperative hemodynamic instability.”1 Although today’s PAAD is focused on adults and adult perioperative care, the recommendations are equally important in pediatric anesthesia practice. I asked Drs. Ethan Sanford and Justin Lockman, our quadruple boarded members of the PAAD’s Executive Council, to review this article for our PAAD readership. Myron Yaster MD
Original article
Scott MJ; APSF Hemodynamic Instability Writing Group. Perioperative Patients With Hemodynamic Instability: Consensus Recommendations of the Anesthesia Patient Safety Foundation. Anesth Analg. 2023 Dec 28. doi: 10.1213/ANE.0000000000006789. Epub ahead of print. PMID: 38153876.
Anesthesia trainees are conditioned through a Pavlovian mechanism to glance at the monitor after the beep of a new blood pressure. Core to our field, and embedded in our collective psyche, is the ever-present awareness of the physiologic state of patients. Indeed, the simplest explanation of what we do is captured by the statement “The air goes in and out, and the blood goes round and round.” But how do we know the latter is happening? After all, blood pressure is at best a poor surrogate for cardiac output (CO) – recall that CO = BP x SVR, and that patients can have low, normal, or high CO with low, normal, or high BP. And while we are often called to the OR or the ICU for concerns about “soft” blood pressures, we don’t actually know what a “hard” blood pressure would look like; we always ask people to use the language they mean (hypotension, not soft BP). But even assuming one trusts that BP represents anything meaningful about CO, today’s PAAD article by Scott et al.1 is unsettling as it highlights just how much we still don’t know about blood pressure and oxygen delivery.
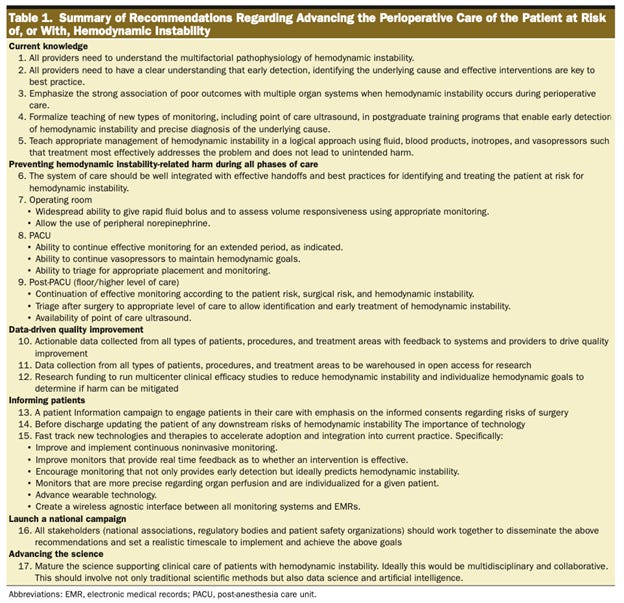
Scott et al. ambitiously summarize our current understanding of hemodynamics, identify deficits in our knowledge, and advocate for greater engagement in preventing, treating, and studying hemodynamic instability-related harm.1 The recommendations do not specifically address children, because the quality and quantity of evidence to support pediatric recommendations in this realm is even lower than in adults. Still, we think this is important and fascinating stuff!
Many of the general principles advocated in the article are applicable to infants, children, and adolescents. The first domain addressed is defining hemodynamic instability. In pediatrics, current practice consists of monitoring and treating largely based on historical blood pressure measurements in healthy children. More recently, normal ranges have been defined for children in the operating room2 and for neonates early in life3 (see this great neonatal BP calculator
https://bloodpressure-neonate.com/ )
So what blood pressure is too low? In adults, the PAAD article refers to large population data demonstrating increasing morbidity/mortality associated with mean arterial blood pressure (MAP) less than 65 mmHg. The odds of poor outcomes increase as magnitude and duration of hypotension increases, as shown in Table 2, reproduced below. In children, secondary analysis of the GAS study demonstrated an alarming incidence of hypotension in infants undergoing general anesthesia (49% had MAP less than 35 mmHg), leading some to wonder about the quality of anesthetic care – but the clinical outcomes of the general anesthesia group were similar to regional anesthesia where hypotension was less common.4 Additionally, a multicenter analysis of blood pressure minimums associated with kidney injury failed to demonstrate blood pressure thresholds for harm in infants and children undergoing noncardiac surgery.5

These data suggest that while improved nomograms for pediatric blood pressure under anesthesia exist, we don’t know when oxygen/substrate delivery to tissues is compromised (i.e., when a shock state exists) or how long this state must exist to cause temporary or permanent harm. Current practice seems to work for most patients but does not illuminate when, or which of, our patients are at risk. Low blood pressure alone may not predict organ injury because CO is likely more important than BP alone. Conversely, a “normal” blood pressure may not be adequate in certain disease states. Static blood pressure measurements simply do not account for the complex factors that impact substrate delivery. Vascular autoregulation, cellular metabolic rates, and downstream venous pressures (i.e., calculated perfusion pressure) are not reflected in blood pressure alone. Not to mention that each organ likely has differential perfusion pressure requirements and autoregulatory abilities, and arterial BP cannot capture this. Each of these factors are also impacted by dynamic changes in illness or surgery including tissue injury, inflammation, sedation, fluid administration, vasoactive use, and more. Sadly, our application of static blood pressure goals to address the complex hemodynamic system is very likely to be inadequate, and we will be flying blind until better end-organ monitoring is available/in use.
How can we improve hemodynamic monitoring? Pulse waveform characteristics and machine learning algorithms have been proposed to amalgamate the large volume of physiologic data to predict who may have poorer outcomes. Additionally, a large discrepancy exists between cardiac ICU/anesthesia and general pediatric ICU/anesthesia in utilization of near-infrared spectroscopy measures of regional tissue blood oxygen saturation (rSO2). High correlation of blood pressure and cerebral rSO2 has been associated with worsened kidney injury, stroke, and mortality outcomes in cardiac surgery. But rSO2 is also imperfect, and improved functional monitors are being developed right now that we hope to use soon. As these new modalities develop, the pediatric anesthesia community would likely best serve our patients by understanding them, discovering their limitations, and incorporating them when feasible. Today’s article advocates for QI and clinical research efforts into these technologies as well.
In the meantime, what can we do to minimize harm caused by hypotension? The authors’ clinical recommendations aren’t surprising but may often not be performed. We encourage you to read the article (also see Table 1, below), but here are our thoughts:
· Vigilantly recognize hemodynamic instability throughout the entire perioperative phase of care, including postoperatively in the PACU and on the inpatient unit/ICU.
· Vital sign and exam changes should be triaged systematically. Cognitive bias often leads anesthesiologists to reject uncommon, more serious causes of hypotension (like anaphylactic and septic shock), but a better mindset would be to rule out these serious life-threatening complications first, not last, to ensure appropriate rapid escalation of care.
· Once emergency is ruled out, a broader differential including common etiologies can be considered, and the ability to treat them should be rapidly available. For example, pediatric anesthesiologists rely heavily on IV fluid administration as an early treatment for hypotension, but do not often look under the drapes for rash or auscultate for bronchospasm, both of which would support anaphylaxis as a cause.
· Have a low threshold to use vasoactives (generally epinephrine in pediatric anesthesia) to improve cardiac output once hypovolemia is ruled out.
Finally, we sincerely hope that a decade from now some of these critical questions have been better answered. We need more research and quality improvement about what constitutes shock in pediatric surgical patients, and about how best to monitor for it. We challenge the SPA community to take this on as an important patient safety issue we can solve together! Email Myron with your thoughts at MYasterster@gmail.com and he will post in a Friday Reader Response.
References
1. Scott MJ. Perioperative Patients With Hemodynamic Instability: Consensus Recommendations of the Anesthesia Patient Safety Foundation. Anesthesia and analgesia. Dec 28 2023;doi:10.1213/ane.0000000000006789
2. de Graaff JC, Pasma W, van Buuren S, et al. Reference Values for Noninvasive Blood Pressure in Children during Anesthesia: A Multicentered Retrospective Observational Cohort Study. Anesthesiology. Nov 2016;125(5):904-913. doi:10.1097/aln.0000000000001310
3. van Zadelhoff AC, Poppe JA, Willemsen S, et al. Age-dependent changes in arterial blood pressure in neonates during the first week of life: reference values and development of a model. British journal of anaesthesia. May 2023;130(5):585-594. doi:10.1016/j.bja.2023.01.024
4. McCann ME, Withington DE, Arnup SJ, et al. Differences in Blood Pressure in Infants After General Anesthesia Compared to Awake Regional Anesthesia (GAS Study-A Prospective Randomized Trial). Anesthesia and analgesia. Sep 2017;125(3):837-845. doi:10.1213/ane.0000000000001870
5. Schacham NY, Chhabada S, Efune PN, et al. Intraoperative Hypotension and Acute Kidney Injury after Noncardiac Surgery in Infants and Children: A Retrospective Cohort Analysis. Anesthesiology. Jan 1 2022;136(1):93-103. doi:10.1097/aln.0000000000004057