
Hocus Pocus
Elaina E. Lin MD, Justin L. Lockman MD MSEd, and Myron Yaster MD

To avoid putting his ear on a female patient's chest to hear her heartbeat, in 1860, French doctor Rene Laennec created the first version of the stethoscope by rolling up a paper tube and using it as a funnel. Today, the stethoscope wrapped around your neck or very visible in your white coat (remember them?) defines to many that you are a doctor.
These days, the stethoscope is becoming more of a symbol or a “stage prop” for many people. In its place, ultrasound and diagnostic imaging have replaced the stethoscope as a diagnostic tool. While we do still think there is a place for stethoscopes (especially for anesthesiologists), we are forced to acknowledge this truism: Most of us are more likely to believe what we can see than what we can hear.
Point-of-care ultrasound (POCUS) is increasingly accepted in pediatric critical care and emergency medicine as a fundamental tool needed to guide the evaluation and treatment of patients.1-3 Similarly, in pediatric anesthesia, the use of ultrasound for both central and peripheral IV placement, as well as for regional anesthesia and neural blockade, is commonplace and increasingly a fundamental skill set. The American Board of Anesthesiology has recognized POCUS as a core skill by adding cardiac and lung POCUS to the Objective Structural Clinical Examination (OSCE), with abdominal POCUS to follow beginning in 2024. This means it is only a matter of time before POCUS will be used routinely in pediatric anesthesia clinical practice to look at cardiac and pulmonary function, intravascular volume status, presence of a pleural effusion, cardiac effusion, pneumothorax, and (we suspect) gastric contents and free fluid in the abdomen. How should training and competency in the obtaining, interpreting, and clinical application of ultrasound be evaluated? How do we assure that older pediatric anesthesiologists become proficient, or that skills learned in training don’t atrophy and deteriorate? In today’s PAAD, Maxson et al. discuss the challenges of POCUS education, certification, and credentialling in the PICU. The operating room is a different environment than the ICU, and presents unique challenges such as limited access to the chest and/or abdomen, and lack of daily rounds where group teaching occurs. Nonetheless, this model is a lesson and road map for us all. Myron Yaster MD
Original article
Maxson IN, Su E, Brown KA, Tcharmtchi MH, Ginsburg S, Bhargava V, Wenger J, Centers GI, Alade KH, Leung SK, Gowda SH, Flores S, Riley A, Thammasitboon S; Pediatric Research Collaborative on Critical Ultrasound (PeRCCUS), a subgroup of the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network. A Program of Assessment Model for Point-of-Care Ultrasound Training for Pediatric Critical Care Providers: A Comprehensive Approach to Enhance Competency-Based Point-of-Care Ultrasound Training. Pediatr Crit Care Med. 2023 Nov 1;24(11):e511-e519. doi: 10.1097/PCC.0000000000003288. Epub 2023 Jun 1. PMID: 37260313.
“Historically, diagnostic medical imaging has largely entailed education of image acquisition and interpretation as separate skills to varying degrees. As POCUS unites these skills, competency assessments that recognize their dynamic incorporation at the bedside is important as studies are often performed, interpreted, and acted upon by a single operator.”1 How can we teach, verify, and maintain these skills or competencies? Who decides when someone (a non-radiologist) is competent to make medical decisions using POCUS? What is the quality control process to ensure accuracy in diagnosis?
“Physicians are increasingly learning about providing health care services through competency based medical education (CBME).4 This is an outcomes-based approach to educational program design and assessment of learners that focuses on the empowerment of learners through their attainment of measurable competencies. Despite advancement toward CBME implementation, consensus definitions on competencies, assessment methods, tailored learning experiences, and heterogeneous implementation have been an impediment to its fulfillment.”1 We have previously written a PAAD about CBME, and we note that these problems are pervasive in CBME.
“Programmatic assessment (PA) is one of the core components of CBME and required for aligning instruction, learning, and assessment practices with learning outcomes. PA highlights the importance of tailored and frequent competency assessment as an essential and planned part of education.”1 In other words: how do we ensure that we build a POCUS education system, which is different from the early adopters “playing around” with ultrasound.
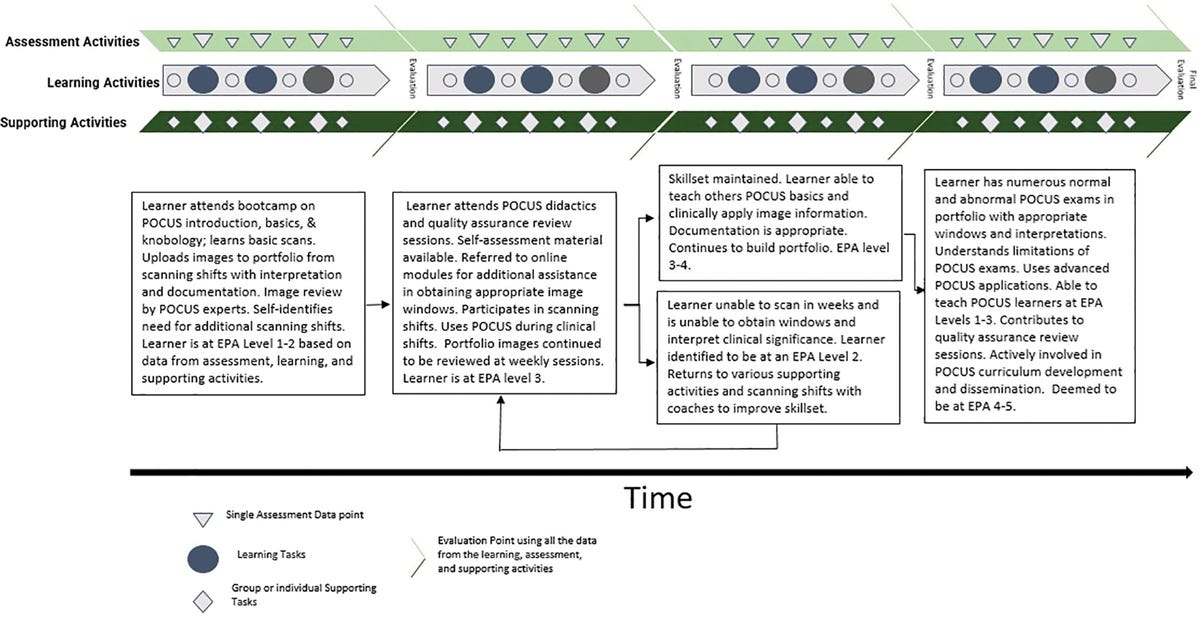
“The four components of a PA model include learning activities, assessment activities, supporting activities, and evaluation activities (figure).
Learning activities are tasks that lead to the acquisition of knowledge. This includes everything from lectures, didactics, and modules to patient encounters, bootcamps, and workshops.
Assessment activities include periodic assessments distributed throughout the curriculum. These assessments are cumulatively evaluated for summative evaluations.
Supporting activities include supplemental educational resources and individualized coaching sessions that support the larger educational mission. These can involve participation in divisional POCUS quality assurance, evidence-based medicine review, or regular textbook readings.
Evaluation activities, conducted by an expert competency committee, determine the learner’s progress by appraising collated data points from the other activities as a summative assessment of competency.”1
It is beyond the scope of a PAAD to go into detail on how such programs can be developed and instituted. We think the Maxson et al.’s article provides a roadmap that will be an invaluable tool to educators and to our professional societies in developing instructional materials, simulation scenarios definitions and demonstration of competencies, and how to logistically implement these programs at both a local and national level. At CHOP, we (EEL and colleagues) have been doing this for over a decade for emergency medicine and critical care medicine, and have an established system of credentialing, skill maintenance, and image review for non-radiologists. Pediatric anesthesiology is a few years behind but catching up fast. We also now are incredibly fortunate enough to have an ultrasound machine in every OR as part of CHOP’s standard setup.
The POCUS train is on the tracks and rolling; we can either drive the engine or be run over. We can’t afford to be left out in developing programs and credentialing for POCUS. This is a real challenge to our profession – and a real opportunity! Should the SPA work to establish shared standards for credentialing in our specialty? How would/could you use ultrasound differently if you had easy access to a machine in every OR? Let Myron know what you think, and he will post in a Friday Reader Response.
References
1. Maxson IN, Su E, Brown KA, Tcharmtchi MH, Ginsburg S, Bhargava V, Wenger J, Centers GI, Alade KH, Leung SK, Gowda SH, Flores S, Riley A, Thammasitboon S: A Program of Assessment Model for Point-of-Care Ultrasound Training for Pediatric Critical Care Providers: A Comprehensive Approach to Enhance Competency-Based Point-of-Care Ultrasound Training. Pediatr Crit Care Med 2023; 24: e511-e519
2. Singh Y, Tissot C, Fraga MV, Yousef N, Cortes RG, Lopez J, Sanchez-de-Toledo J, Brierley J, Colunga JM, Raffaj D, Da Cruz E, Durand P, Kenderessy P, Lang HJ, Nishisaki A, Kneyber MC, Tissieres P, Conlon TW, De Luca D: International evidence-based guidelines on Point of Care Ultrasound (POCUS) for critically ill neonates and children issued by the POCUS Working Group of the European Society of Paediatric and Neonatal Intensive Care (ESPNIC). Crit Care 2020; 24: 65
3. Marin JR, Lewiss RE: Point-of-care ultrasonography by pediatric emergency medicine physicians. Pediatrics 2015; 135: e1113-22
4. Ryan MS, Holmboe ES, Chandra S: Competency-Based Medical Education: Considering Its Past, Present, and a Post-COVID-19 Era. Acad Med 2022; 97: S90-s97