


Heal our world while healing our patients
Galaxy Li, Justin Skowno, Margaret Allen, Elizabeth Hansen

“Hey, what’s that sucking sound?”
“Sevo and nitrous wasted out the scavenger… all 97% of it”
Original Article:
Diane Gordon, Jeffrey Feldman: Environmentally responsible mask induction, Best Practice & Research Clinical Anaesthesiology,
Volume 38, Issue 4, 2024, Pages 321-331, ISSN 1521-6896, https://doi.org/10.1016/j.bpa.2025.02.001.
(https://www.sciencedirect.com/science/article/pii/S1521689625000059)
In their paper, “Environmentally responsible mask induction,”1 Drs. Gordon and Feldman present a call to action for pediatric anesthesiologists to reduce waste and emissions through environmentally conscious inhalation inductions. These authors, both well-known in the field of sustainable anesthesiology, highlight the unique opportunities pediatric anesthesiologists have in reducing the carbon footprint of healthcare.
Drs. Gordon and Feldman used a GasMan (https://www.gasmanweb.com/ ) simulation to model various clinical scenarios and demonstrate the inefficiency of traditional practices and how simple changes can significantly reduce emissions. They analyzed the efficiency of the conventional pediatric practice of sevoflurane induction. After three minutes of 8% sevoflurane and 70% nitrous oxide (N2O) at 10L/min fresh gas flow (FGF), only 3.3% of the sevoflurane and 2.1% of the N2O is effectively delivered to the patient, and the remainder is emitted as unnecessary waste, equivalent to driving 35 miles in a standard gas powered car.
This induction style mirrors what we did for nearly all of our cases during training, primarily due to the historical practice of mask inductions with a predecessor of sevoflurane. Halothane was plagued with risks of cardiovascular depression, dysrhythmias, and laryngospasm, requiring a delicate but deliberate uptitration. Traditionally, N2O was used to provide sedation prior to starting the pungent agent and / or added to increase its update via the second gas effect. Sevoflurane, by comparison, is so much more well-tolerated by children that adding another agent such as N2O is unnecessary. Further, because it is so insoluble compared to halothane, the second gas effect becomes irrelevant.
The art of an inhalation induction is a vital skill for pediatric anesthesiologists, and we owe it to our patients to effectively perform at a high efficacy with minimum detriment on their futures. Fortunately, the authors present four simple strategies to achieve this: stop using N2O, limit fresh gas flow (FGF) to match the patient’s minute ventilation, properly prime the circuit when needed, and reduce FGF as early as possible after induction.
Stop using nitrous oxide
There is no clear evidence that adding nitrous oxide to a sevoflurane induction provides real clinical benefit, but there is significant environmental harm as it is a potent greenhouse gas with 273 times the global warming potential of carbon dioxide over a 100-year time horizon. We already know that avoidance of N2O does not significantly impact induction time or patient behavior.2 Instead, we place a scent in the mask and provide a nice distraction!
Decrease fresh gas flow for induction
Because rebreathing within a circle system is not desirable for the purposes of an efficient inhalation induction, it can be eliminated when FGF is greater than or equal to minute ventilation. By using weight-based FGF limits (based on 150 mL/kg) for inhalation induction, instead of historically high flows, clinicians can achieve similar clinical outcomes while improving efficiency from the 3.3% in the example above, to over 50% with the most efficient examples where FGF is reduced early in the induction process. Close monitoring of fluctuations in anesthetic concentration and fraction of inspired oxygen is essential at lower flows.3,4 For a deeper dive see the Society for Pediatric Anesthesia’s one pager: Low flow anesthesia in pediatric patients https://pedsanesthesia.org/wp-content/uploads/2021/08/Low-Flow-Anesthesia-in-Pediatric-Patients.pdf
Properly prime the circuit if needed
In situations where a high concentration of sevoflurane is required from the onset, the circuit should be appropriately primed to minimize waste. The authors recommend that the reservoir bag be emptied when the vaporizer is turned on, then applying the mask to the patient once the reservoir bag is full to optimize patient comfort and speed of induction.
Reduce intraoperative FGF
Decreasing FGF after induction of anesthesia takes advantage of rebreathing to minimize environmental pollution from scavenged gases and is a well understood (but perhaps not well practiced) step. Gordon and Feldman effectively demonstrate the environmental utility of reducing FGFs, but also clearly show that maintenance flows cannot be safely reduced enough to compensate for the waste created by the traditional high FGF induction. Reducing FGF for earlier equilibration is key to optimizing both the concentration of sevoflurane and minimizing waste during maintenance.
Gordon and Feldman graph out the following scenarios to explain reductions in waste. Efficiency is 6.5% after decreasing fresh gas flows to 1 L/min after 3 minute induction of 8% sevoflurane at 10 L/min. Efficiency increases to 23% when fresh gas flows are initially set at 1.5L/min and then decreased to 0.5 L/min after 30 seconds. Efficiency increases to 51% when fresh gas flows are initially set at 1.5L/min and then decreased to 0.5 L/min after 30 seconds and then further decreased to 0.1 L/min for the remainder of the hour.
Drs Gordon and Feldman encourage practitioners to understand the historical reasoning behind how inhalation inductions have evolved to the current state, and why that practice should be updated to optimize patient care in the setting of environmental stewardship with modern inhalation anesthetics. They responsibly disclose that despite the sophisticated GasMan simulations, its quantitative data does not predict identical clinical results. Unsurprisingly, they also prioritize increasing FGF if maintaining an effective mask seal proves difficult and treating any sevoflurane-induced hypotension (by reducing sevoflurane concentration quickly using higher FGF) over the goal of environmental protection, such as during the post-induction, pre-incision period. As you consider practice changes, we encourage you to heal our world together as we heal our patients, one at a time.
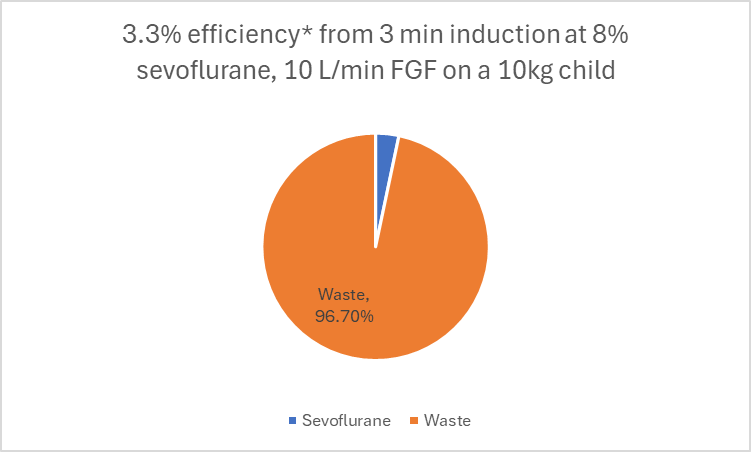
3.3% of Sevoflurane is effectively delivered to a 10kg child after 3 minutes of 10 L/min fresh gas flow at 8% Sevoflurane, leaving 96.7% of the inhaled agent to waste, based on a Gasman simulation model.
The strategies discussed in today’s PAAD are only a few that are outlined in the American Society of Anesthesiologists’ Statement on Greening the OR and Perioperative Arena.
Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Gordon D, Feldman J: Environmentally responsible mask induction. Best Practice & Research Clinical Anaesthesiology 2024; 38: 321–331
2. Isserman RS, Yuan I, Elliott EM, Muhly WT, Iyer RS, Farrell HA, Varallo DA, Georgostathi G, Richter AG, Stiso J, Tsui FR, Feldman JM: Reducing the environmental impact of mask inductions in children: A quality improvement report. Paediatr Anaesth 2023; 33: 728–735
3. Feldman JM: Managing fresh gas flow to reduce environmental contamination. Anesth Analg 2012; 114: 1093–101
4. Kennedy RR, Hendrickx JF, Feldman JM: There are no dragons: Low-flow anaesthesia with sevoflurane is safe. Anaesth Intensive Care 2019; 47: 223–225