
First-Attempt Success in Ultrasound-Guided vs Standard Peripheral Intravenous Catheter Insertion in Pediatric Patients
Myron Yaster MD, Allison Kinder Ross MD, and Lynne G. Maxwell MD

We’ve all been there…you can’t cannulate a vein despite multiple IV start attempts. You call for help and as the cavalry arrives, a quick glance shows a pile of spent IV catheter detritus and “bullet holes” on all 4 of the patient’s extremities and maybe even the scalp. You call for the ultrasound machine and while it is being set up a vein is cannulated by one your colleagues the old-fashioned way, by palpation, skill, and luck. In 2025 should we still be placing IVs the old-fashioned way or should our first attempt be with ultrasound guidance? This is heresy for most of you particularly old-timers, who pride themselves on their IV placement expertise but are we letting our egos get in the way of a better approach? Indeed, is there DATA to guide our practice? In today’s PAAD, Kleidon et al.1 performed a large, randomized controlled, single center trial to find out.
Original article
Kleidon TM, Schults JA, Royle RH, Gibson V, Ware RS, Andresen E, Cattanach P, Dean A, Pitt C, Ramstedt M, Byrnes J, Nelmes P, Rickard CM, Ullman AJ. First-Attempt Success in Ultrasound-Guided vs Standard Peripheral Intravenous Catheter Insertion: The EPIC Superiority Randomized Clinical Trial. JAMA Pediatr. 2025 Jan 27:e245581. doi: 10.1001/jamapediatrics.2024.5581. Epub ahead of print. PMID: 39869351; PMCID: PMC11773401.
“Traditional PIVC insertion (standard, or landmark, technique) relies on vein palpation and visualization. This subjective method depends on clinician skill and can be challenging. Children with difficult intravenous access (DIVA) due to age (history of prematurity, being aged <3 years), chronicity (severe comorbidities, prolonged hospitalization), and appearance (few palpable and visible veins) present additional challenges,2,3 highlighting the inadequacy of current practice to meet the needs and abilities of all patients and clinicians. Ultrasound guidance (USG) offers an alternative, providing real-time visualization of the vein (size, depth, abnormalities such as stenosis) and needle tip and enhancing insertion accuracy.”1
“Clinicians use ultrasound guidance intuitively for high-risk children, while standard techniques are used for children with unknown or moderate risk until insertion fails. To comprehensively evaluate the broader utility of USG PIVC insertion in the context of a nonspecialist workforce, a rigorous randomized clinical trial was conducted to evaluate its effectiveness and safety across all levels of insertion difficulty.”1
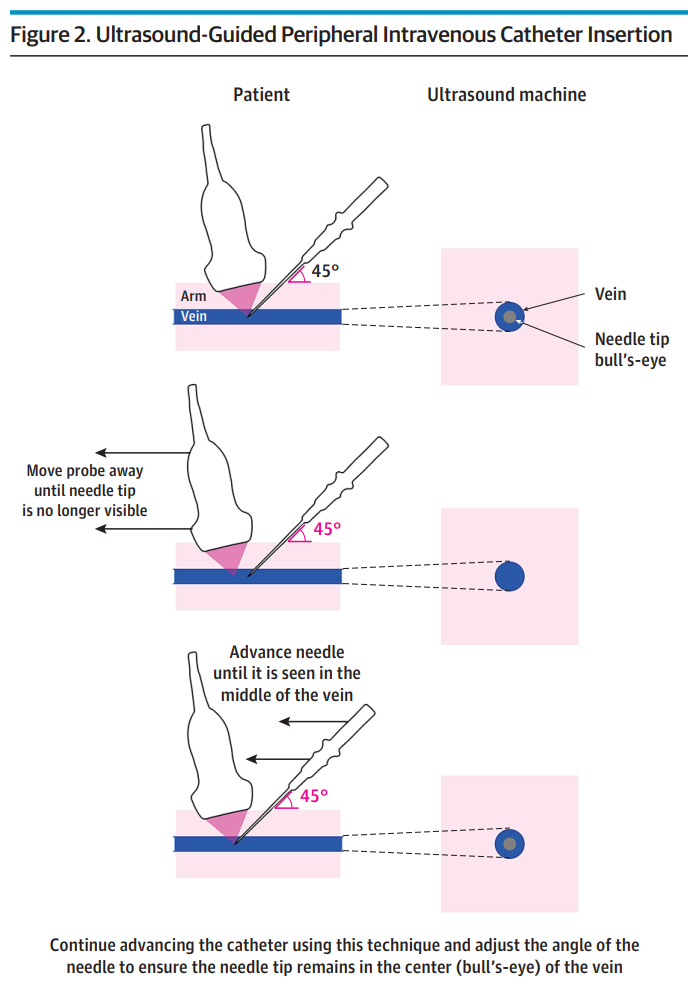
First and foremost, this study was NOT performed in the OR or by anesthesia personnel. “In this trial, clinicians performed procedures only if they were competent and had recent practice in the randomized technique (standard or USG). Children assigned to the standard technique (palpation and visualization) served as the control group. These PIVCs were inserted by a registered nurse or medical officer with demonstrated proficiency and recency of practice in standard PIVC insertion technique as per local hospital policy.”1 All USG PIVCs were inserted with an out of plane technique (figure).
OK, what did they find? “A total of 164 children were randomly assigned to ultrasound-guided insertion (n = 84) or standard care (n = 80), with 81 (96.4%) and 78 (97.5%) receiving their allocated intervention, respectively. The median (IQR) age was 24 (10-120) months, and 93 children (56.7%) were male. First-time insertion success was higher with ultrasound-guided PIVC insertion (72 children [85.7%]) compared with standard technique (26 children [32.5%]) (risk difference [RD], 53.6%; 95% CI, 41.7%-65.4%; P < .001). The authors conclude that ultrasound guidance PIV catheter insertion improves first-time insertion success across all risk categories in pediatrics, supporting the widespread adoption of ultrasound-guided PIVC insertion in children.”1
Sounds reasonable enough, but a 37.5% successful insertion rate appears to us to be preposterously low! Or have the skill sets for our colleagues in nursing and pediatrics/general medicine fallen so low that this “success” rate is actually accurate? We think that if this study were done in the Operating Rooms by fellowship trained anesthesiologists the results would be far different. However those of us who did pediatric residency cannot forget the difficulty of IV placement in a screaming, writhing child in the emergency room and are grateful every day for having the blessing of placing IV’s in a sleeping, motionless child, whether by palpation/visualization or with ultrasound assistance. Thus, this is an ideal opportunity for one or several of you to perform this controlled randomized controlled trial in your practice.
Part of this difference in success rate could be attributed to the practitioners who are performing the insertion. Although the children were randomized to the 2 groups (USG vs standard), the practitioners were not. There was only one vascular nurse practitioner in the standard group whereas 75% of the practitioners in the standard group were medical officers, presumably in a variety of stages of training and many (?most) without the years of expertise of a vascular access nurse. The “real life” scenario presented in this article is eye opening and does make one consider how best to manage children who are at the mercy of a variety of staff with varying levels of experience, skill and luck. It is important therefore not to make sweeping changes to intravenous access protocols without considering your own institution’s staffing, processes and procedures.
What do you think of these results and its implications? Send your thoughts and comments to Myron who will post in a Friday reader response.
References
1. Kleidon TM, Schults JA, Royle RH, Gibson V, Ware RS, Andresen E, Cattanach P, Dean A, Pitt C, Ramstedt M, Byrnes J, Nelmes P, Rickard CM, Ullman AJ. First-Attempt Success in Ultrasound-Guided vs Standard Peripheral Intravenous Catheter Insertion: The EPIC Superiority Randomized Clinical Trial. JAMA Pediatr. 2025 Jan 27:e245581. doi: 10.1001/jamapediatrics.2024.5581. Epub ahead of print. PMID: 39869351; PMCID: PMC11773401.
2. Bahl A, Johnson S, Alsbrooks K, Mares A, Gala S, Hoerauf K. Defining difficult intravenous access (DIVA): A systematic review. J Vasc Access. 2021 Nov 17:11297298211059648. doi: 10.1177/11297298211059648. Epub ahead of print. PMID: 34789023.
3. Schults JA, Kleidon TM, Gibson V, Ware RS, Monteagle E, Paterson R, Charles K, Keys A, McBride CA, McTaggart S, Lawton B, Macfarlane F, Sells C, Rickard CM, Ullman AJ. Improving peripheral venous cannula insertion in children: a mixed methods study to develop the DIVA key. BMC Health Serv Res. 2022 Feb 17;22(1):220. doi: 10.1186/s12913-022-07605-2. PMID: 35177041; PMCID: PMC8851754.