
External ventricular drains: What the pediatric anesthesiologist should know
Myron Yaster MD, Justin Hamrick MD, and Justin L. Lockman MD MSEd

Original article
Lele AV, Bebawy JF, Takala R. The External Ventricular Drain Safety Campaign: A Global Patient Safety Initiative of the Society for Neuroscience in Anesthesiology and Critical Care. J Neurosurg Anesthesiol. 2024 Jul 24. doi: 10.1097/ANA.0000000000000982. Epub ahead of print. PMID: 39051910.
Many patients with hydrocephalous require diversion of cerebrospinal fluid (CSF) with external ventricular drains (EVDs) to reduce the risk of life-threatening increases in intracranial pressure (ICP) or to relieve existing intracranial hypertension and impending cerebral herniation. Others have EVDs placed temporarily while being treated for infection of their permanent ventriculoperitoneal shunts. We often deal with these drains in transport to and from the ICUs and during neurosurgical and non-neurosurgical procedures as well as imaging studies. Unfortunately, most of us have received little to no education about the prevention of under- or over-drainage of CSF, accidental disconnection or dislodgement, or infectious complications. Further, during intrahospital transport, these drains are sometimes clamped (potentially causing dramatic increases in ICP) – but how is the anesthesiologist to know when this is a risk and when it is not?
In today’s PAAD, Lele and Bebawy1 discuss new guidelines for the perioperative care of patients with EVDs developed by the Society for Neuroscience in Anesthesiology and Critical Care (SNACC).2 They have created a free, on-line training module based on these guidelines.3 As discussed in many previous PAADs, guidelines may be perfectly written but how do you get anesthesiologists to change practice and follow them? Just think about hand washing or better ways to secure an IV (PAAD June 13, 2024 https://ronlitman.substack.com/p/implementation-science )? [As a side note, this is where implementation science enters, and we are excited to announce expansion of the PAAD’s Executive Council to include Drs. Lynn Martin, Todd Glenski, Kim Strupp, David Buck, Megha Kanjia and Odi Ehie as regular reviewiers for articles on Implementation Science and Quality Improvement (and related topics) going forward for the PAAD readership.]
Back to today’s article… Lele and Bebawy report that despite these new guidelines and development of training modules, “variations in hospital policies and procedures promulgate [the clamping of EVDs even when it’s not safe]… exposing patients to potential harm.” 1,4 Further, awareness of the guidelines and training module, they report, remains low. Thus, SNACC is embarking on a global patient safety initiative: “The EVD Safety Campaign,” including a knowledge hub approved by the SNACC Board of Directors that can be accessed via the SNACC website (https://snacc.org/external-ventricular-drain-campaign/). “The knowledge hub contains portable digital formats for the SNACC EVD guidelines, the SNACC educational document, a policy and procedure template, and a list of perioperative quality metrics that can be downloaded free of charge. An educational video and an EVD self-assessment quiz are also available.”1
To be clear, these guidelines were primarily written for ADULT patients. How do they stack up for pediatric patients? These guidelines provide a good foundation for the perioperative care of any patient with an EVD. However, there are some differences. First, EVDs are usually placed for one of two reasons in pediatrics: (1) Temporary diversion of CSF in a patient with an infected longer term shunt (i.e., VP shunt) or (2) Acutely in a patient with increased intracranial pressure where it may be used as both an ICP monitor AND a treatment modality (by drainage of CSF from the intracranial space). These two situations provide unique and distinct challenges for the pediatric anesthesiologist in the perioperative period.
As stated in the published guidelines2, “Parts of evaluation that are unique to EVDs include reviewing indication for placement, relevant history, medications given, ICP trends, qualitative evaluation of components of ICP waveforms, and any data available from EVD clamp trials.” These components will give you a good indication of the ICP compliance curve, where the patient is currently located on it, and how the patient will react to even brief EVD clamping and alternative positioning during transport and the procedure. Critical to this issue is understanding that symptomatology is not linear: patients do not always have a headache before they vomit, or vomit before they spike their ICP. Some patients are already on the steep part of the curve and can spike their ICP nearly immediately on EVD clamping.
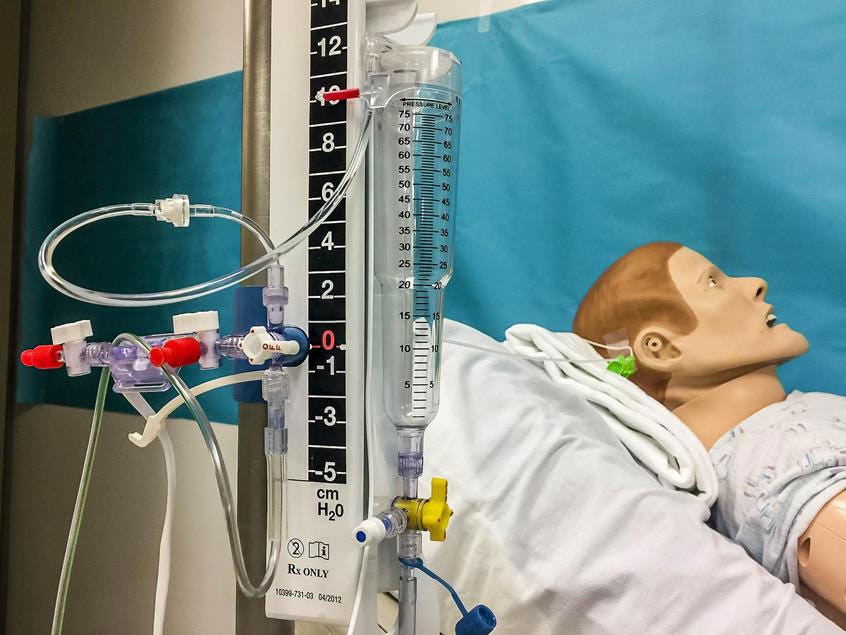
For monitoring ICP during cases, remember that EVDs are usually “leveled” at the external auditory meatus (position of the circle of Willis), and then may be elevated 0-20 cm above that. It is also important to understand EVD drain dynamics. How much has been drained per hour in the ICU? In adults this usually matches the CSF production (10-20 mL/hr) but may be different in pediatrics and for each patient depending on the indication for the EVD. As with everything else in anesthesia, we should probably keep doing whatever the patient has required for homeostasis! Overdrainage may result in a bridging vein tear, and ultimately lead to a subdural bleed. This is especially important in a pediatric population that may be agitated in the perioperative period causing momentary spikes in the ICP which themselves may result in overdrainage if not monitored closely. Some of these patients require intermittent clamping of an EVD after the prescribed amount per hour of CSF has been drained. Again, tolerance by patients of any period of clamping depends upon the primary reason for placement of EVD, ICP trends, and dependency on external CSF diversion. Patients at risk for clamp failure include those dependent on external CSF diversion, such as occurring with acute hydrocephalus, and in situations of elevated ICP.2
The ICP waveform itself is extremely important in the diagnosis of ICP compliance but is beyond the scope of this review (foreshadowing for later?). The main question to ask is “how is the patient going to respond to what we need to do in the perioperative period?”. These include changes in position (many times from head of bed elevated 30 degrees to supine/flat positioning), changes in ventilation, changes in hemodynamics (i.e., cerebral perfusion pressure), EVD clamping needed during transport and position changes, etc. This all may be compounded by the fact that some locations may be incapable of monitoring ICP during the procedure (CT, MRI, or others) due to technical limitations.
As always, clear and concise communication with the entire team is paramount in the care of these patients. What do the surgeons or imaging teams need (position, time, etc.)? What is the PICU experience for these patients? What has worked and what hasn’t worked? Has the ICP gotten worse or better over time? Is the timing of the procedure appropriate?
The main questions to ask include:
What was the indication for EVD placement?
What are your current uses for the EVD? Monitoring ICP alone? CSF diversion for an infected VP shunt awaiting infectious clearance for replacement? Monitoring and treatment for increased ICP (as in a patient with TBI)?
Is there a current goal for CSF drainage (mL/hr)? What do you do after that goal is reached?
What is the patient’s ICP compliance curve? How did they respond to a clamp trial (if performed)? How do they respond to supine positioning?
Any issues with the EVD (clotting requiring flushing, etc.)?
What height is it leveled at? (usually 0-20 cm above level)
Do you feel comfortable and knowledgeable about EVDs? We encourage you to explore the free SNACC resources mentioned here. Because the management of EVDs is an essential part of practice, we think that this would be an ideal topic for a future PEDx talk at a SPA meeting. Send your thoughts and comments to Myron at myasterster@gmail.com who will post in a Friday Reader Response.
References
1. Lele AV, Bebawy JF, Takala R. The External Ventricular Drain Safety Campaign: A Global Patient Safety Initiative of the Society for Neuroscience in Anesthesiology and Critical Care. Journal of neurosurgical anesthesiology 2024 (In eng). DOI: 10.1097/ana.0000000000000982.
2. Lele AV, Hoefnagel AL, Schloemerkemper N, et al. Perioperative Management of Adult Patients With External Ventricular and Lumbar Drains: Guidelines From the Society for Neuroscience in Anesthesiology and Critical Care. Journal of neurosurgical anesthesiology 2017;29(3):191-210. (In eng). DOI: 10.1097/ana.0000000000000407.
3. Lele AV, Takala RSK, Athiraman U, et al. Implementation of an Online External Ventricular Drain Training Module-An Educational Initiative to Improve Proficiency of Perioperative Health Care Providers: Results of a Retrospective Study. Journal of neurosurgical anesthesiology 2023;35(2):201-207. (In eng). DOI: 10.1097/ana.0000000000000815.
4. Thamjamrassri T, Yuwapattanawong K, Chanthima P, Vavilala MS, Lele AV. A Narrative Review of the Published Literature, Hospital Practices, and Policies Related to External Ventricular Drains in the United States: The External Ventricular Drain Publications, Practices, and Policies (EVDPoP) Study. Journal of neurosurgical anesthesiology 2022;34(1):21-28. (In eng). DOI: 10.1097/ana.0000000000000694.