


Celecoxib (Celebrex) and post tonsillectomy bleeding
Myron Yaster MD, Constance L. Monitto MD, Aaron Low, MD, and Lynn D. Martin MD, MBA

This PAAD was first published on August 6, 2024
Tonsillectomy, one of the most common surgical procedures performed in children, is, unfortunately, associated with a number of postoperative complications, most notably postoperative hemorrhage. Further, moderate-to-severe pain following tonsillectomy is expected, can last for over a week, and can impair oral intake leading, at times, to dehydration. Many children who undergo tonsillectomy do so for the treatment of obstructive sleep apnea, and as such may be at increased risk of opioid-induced respiratory depression. Hence, there is a strong emphasis among otolaryngologists on providing opioid-sparing analgesics such as acetaminophen and NSAIDs as first-line analgesic therapy at discharge. However, the impact of nonselective NSAIDs on the frequency and quality of post-tonsillectomy hemorrhage (PTH) remains open to debate. In today’s PAAD So et al.1 wondered if managing pain with celecoxib (Celebrex, Pfizer), a selective COX-2 inhibitor, would impact the risk of PTH. I’ve asked Drs. Aaron Low and Lynn Martin of Seattle Children's Hospital and Dr. Constance Monitto of Johns Hopkins Hospital to help. Myron Yaster MD
Original article
So V, Radhakrishnan D, MacCormick J, Webster RJ, Tsampalieros A, Zitikyte G, Ripley A, Murto K. Does Celecoxib Prescription for Pain Management Affect Post-tonsillectomy Hemorrhage Requiring Surgery? A Retrospective Observational Cohort Study. Anesthesiology. 2024 Aug 1;141(2):313-325. doi: 10.1097/ALN.0000000000005032. PMID: 38684054.
Tonsillectomy with or without adenoidectomy is among the most common surgical procedures performed in children. In North America, indications for surgery include sleep disordered breathing, obstructive sleep apnea, and/or recurrent infection. (I (MY) would cynically add presence of insurance).
Because of concerns regarding the risk of opioid-induced respiratory depression in children with obstructive sleep apnea, and further fueled by attempts to spare opioid administration related in part to the opioid epidemic, pain management following tonsillectomy has increasingly relied on administration of acetaminophen and non-selective NSAIDs to minimize opioid consumption while providing adequate levels of analgesia.2,3 However, the “main mechanism of action of NSAIDs is the inhibition of cyclooxygenase enzymes including COX-1 and COX-2, which can affect bleeding risk through COX-1-mediated effects on hemostasis and platelet function.4”1
While prior studies and systematic reviews have generally not found the frequency of PTH to be significantly increased when nonselective NSAIDs are prescribed, to date there is insufficient evidence to definitively discount bleeding risks in children. In addition, some evidence has suggested that even if the incidence is not increased, severity of bleeding may be increased with ibuprofen administration.5 Thus, So and colleagues questioned whether using celecoxib, a selective oral COX-2 inhibitor which has minimal if any effects on platelet adhesion and aggregation, would impact the risk of postoperative hemorrhage requiring surgery following tonsillectomy.
The authors completed a retrospective, observational cohort study involving 5,846 children under 18 years of age from Eastern (Ottawa) Ontario, Canada, who underwent tonsillectomy between January 2007 and December 2017. Tonsillectomies were “performed by 23 ear, nose, and throat surgeons (otolaryngologists) whose primary practice was in a tertiary adult center (43.4%), in a community practice (34.8%), or at Children’s Hospital of Eastern Ontario (21.7%).”1 Starting in 2009, oral celecoxib became the standard of care for post-tonsillectomy pain, and prescribing frequency increased such that celecoxib was prescribed to 1,644 patients (23%) during the study period. Celecoxib was prepared by the hospital pharmacy as a 10 mg/mL oral suspension,5 and patients were given a 6 mg/kg loading dose preoperatively (maximum 550 mg), and prescribed 3 mg/kg twice daily, initially for 3 days and subsequently for 10 days following surgery.1 Of note, patients who did not receive celecoxib (either pre- or postoperatively), many of whom were cared for prior to 2010, were prescribed acetaminophen and an oral opioid (either codeine or liquid morphine) at discharge, but not a non-selective COX inhibitor such as ibuprofen or ketorolac.
The authors found that in their cohort, PTH requiring surgery occurred in 1.7% of patients. Most hemorrhages occurred at a time that coincided with fibrin clot separation and rapid capillary development in the vascular stoma being vulnerable to bleeding (median 5 days, IQR, 2 to 8). In addition, they found no significant difference in the proportion of PTH requiring surgery in children prescribed celecoxib (1.94%, 95% CI, 1.36 to 2.75) versus those not prescribed celecoxib (1.62%, 95% CI, 1.25 to 2.10).1 Adjusting for surgeon, patient weight, surgery time and total celecoxib dose prescribed at discharge did not alter this finding. These results led the authors to conclude that their large retrospective cohort study provided evidence for the safety of celecoxib administered to children to treat post-tonsillectomy pain, but that confirmation with a multisite randomized controlled trial was still required.1
When drawing conclusions from this study there are several issues to consider. First, the long-time frame of this retrospective study (11 years) likely coincided with evolution in surgical techniques that could have significant impact on the bleeding rate. In Seattle, the intracapsular technique (n=407) versus all other surgical techniques (n=5,764) has a lower PACU Max Pain Score (3.1 vs 3.8), 30-day all-cause hospital readmission rate (12.3 vs 38.3 per 1000 cases), same day return to OR (0.00% vs 0.17%), and 30-day return to OR (0.0% vs 1.5%).
Next, what degree of post-tonsillectomy bleeding is the most relevant study – and clinical – endpoint on which to base management decisions? Options include type 1 PTH, in which bleeding is observed at home or assessed in an emergency department without further intervention; type 2 PTH, which requires readmission for observation, and type 3 PTH, which requires surgical intervention. The authors chose to address only type 3 hemorrhages here, probably because those are the most clinically concerning, but also because their retrospective study approach did not provide complete data on other, less severe types of hemorrhage.
Interestingly, Mudd and colleagues at Children’s Hospital of Philadelphia took endpoint choice a step further in a 2017 retrospective study.6 They found no significant increased risk of PTH requiring surgery associated with postoperative ibuprofen use, but using transfusion rates as a surrogate for severity of PTH they found that transfusion rates increased by more than three-fold among ibuprofen users compared with nonusers (adjusted OR, 3.16; 95% CI, 1.01 to 9.91). Further, their 95% CI upper limit suggested the difference could be nearly 10 times greater and supported their decision to transition their post-tonsillectomy NSAID prescribing away from ibuprofen to celecoxib. Here at Seattle, 133 PTH patients receiving intraoperative ketorolac required return to the OR, of which 6 required transfusion. This represents a transfusion rate of 4.5%, similar to the rate of transfusion (4.4%) of patients not receiving ibuprofen in Mudd et al’s study.
Finally, risk tolerance in NSAID prescribing remains variable at different pediatric institutions. In Seattle non-specific NSAIDs were routinely introduced into the perioperative management of tonsillectomy pain in 9/2018, including administration of ketorolac at the end of surgery for opioid sparing.3

We have 3,324 patients receiving intraoperative ketorolac and 2,843 receiving no ketorolac. Data from these two cohorts of patients regardless of surgical technique are presented in the table.
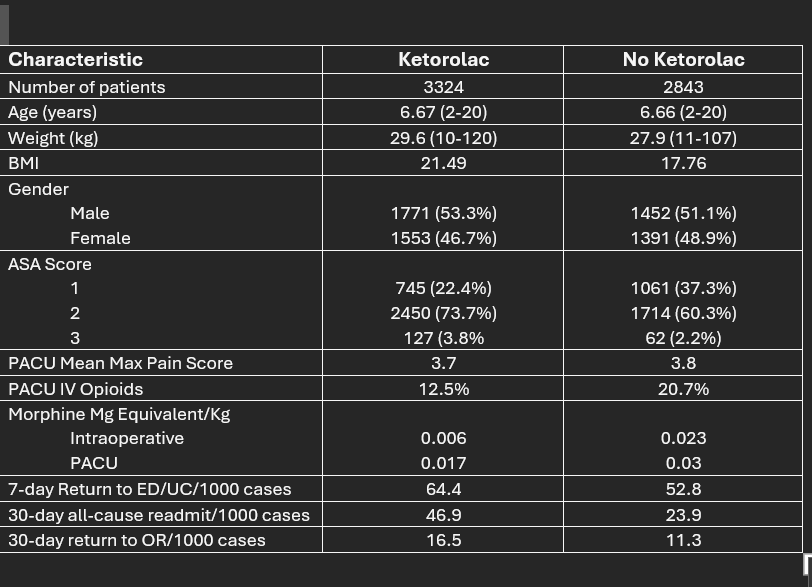
The 7-day ED/UC visit could be thought of as PTH 1 while 30-day all cause readmission rate as PTH 2 and 30-day reoperation as PTH 3. The PTH 3 rate requiring surgical intervention was not different.
The all-cause readmission rate was increased, but other causes for admission (pain, dehydration) can’t be excluded.
On the other hand, in Baltimore, concern for bleeding risk related to ketorolac has led to almost universal avoidance of ketorolac in tonsillectomy patients. Rather, children are routinely administered ibuprofen in the PACU, discharged home on acetaminophen and ibuprofen – and almost never given an opioid prescription for severe pain. In speaking to the chief pediatric otolaryngologist at Hopkins, he felt no compelling reason to transition away from ibuprofen given the current level of evidence.
Another limitation in assessing the safety of celecoxib administration based on this study is that what was actually measured was not celecoxib administration, but rather the provision of a celecoxib prescription. The authors previously found 96% compliance in a smaller randomized controlled study looking at celecoxib’s analgesic efficacy and impact on functional recovery in pediatric patients undergoing adenotonsillectomy,7 but compliance rates here are not known.
Finally, readers may want to consider how celecoxib fits into their practice. Celecoxib is prescribed for children down to 2 years of age for pain related to rheumatologic disease, but its use for treatment of acute postoperative pain in children is off label. Further, kinetics in young children differ from those in adults, leaving optimal dose and dosing interval open to debate.8 Unlike this study in which the hospital pharmacy prepared an oral formulation for dispensing, liquid formulations are not readily available in the US, but capsules can be opened and their contents mixed with food or water to facilitate administration. While not routinely prescribed following tonsillectomy in Baltimore, the Pediatric Acute Pain Service does prescribe celecoxib in certain circumstances. As a selective COX-2 inhibitor, its impact on platelet function is minimal and hence it is at times prescribed to oncology patients, though not those with extremely low platelet levels, much as choline magnesium trisalicylate (Trilisate) was in the past. In addition, due to surgical preference, it is the NSAID of choice when transitioning to oral analgesics following posterior spinal fusion surgery.
What is your experience with celecoxib and your analgesic management paradigm following tonsillectomy in children? Send your thoughts to Myron, who will post in a Friday reader response.
References
1. So V, Radhakrishnan D, MacCormick J, et al. Does Celecoxib Prescription for Pain Management Affect Post-tonsillectomy Hemorrhage Requiring Surgery? A Retrospective Observational Cohort Study. Anesthesiology 2024;141(2):313-325. DOI: 10.1097/aln.0000000000005032.
2. Amin SN, Thompson T, Wang X, et al. Reducing Pediatric Posttonsillectomy Opioid Prescribing: A Quality Improvement Initiative. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery 2024;170(2):610-617. (In eng). DOI: 10.1002/ohn.534.
3. Martin LD, Franz AM, Rampersad SE, et al. Outcomes for 41 260 pediatric surgical patients with opioid-free anesthesia: One center's experience. Pediatric Anesthesia 2023;33(9):699-709. DOI: https://doi.org/10.1111/pan.14705.
4. Schafer AI. Effects of nonsteroidal antiinflammatory drugs on platelet function and systemic hemostasis. JClinPharmacol 1995;35(3):209-219.
5. Donnelly RF, Pascuet E, Ma C, Vaillancourt R. Stability of celecoxib oral suspension. The Canadian journal of hospital pharmacy 2009;62(6):464-8. (In eng). DOI: 10.4212/cjhp.v62i6.844.
6. Mudd PA, Thottathil P, Giordano T, et al. Association Between Ibuprofen Use and Severity of Surgically Managed Posttonsillectomy Hemorrhage. JAMA Otolaryngol Head Neck Surg 2017;143(7):712-717. (In eng). DOI: 10.1001/jamaoto.2016.3839.
7. Murto K, Lamontagne C, McFaul C, et al. Celecoxib pharmacogenetics and pediatric adenotonsillectomy: a double-blinded randomized controlled study. Canadian journal of anaesthesia = Journal canadien d'anesthesie 2015;62(7):785-97. (In eng). DOI: 10.1007/s12630-015-0376-1.
8. Stempak D, Gammon J, Klein J, Koren G, Baruchel S. Single-dose and steady-state pharmacokinetics of celecoxib in children. Clinical pharmacology and therapeutics 2002;72(5):490-7. (In eng). DOI: 10.1067/mcp.2002.129322.