


Checklist for intraoperative handoffs: does less improv improve harmony?
Myron Yaster MD, Jamie McElrath Schwartz MD, and Eugenie S. Heitmiller MD

When I think back to some of the most important changes that have occurred in the clinical practice of pediatric anesthesia over the past 2 decades, few have had as much impact on over all quality and safety as the institutionalization of checklists in perioperative management. Ok, many of you will argue that ultrasonography for central line insertion, difficult IV placement and peripheral neural blockade, or video laryngoscopy for difficult airway management, or even the widespread adoption of the electronic billing, I mean electronic medical record (EMR), were more important. I disagree - standardization really matters and has a much wider scope. Just think about how we place central lines today. Chlorhexidine prep, full patient body sterile draping, a cart containing all the supplies, OR personnel who could quite literally stop the procedure if you didn’t follow the checklist, yada yada yada…you get the picture. Admittedly, I hated this and felt like a prisoner/hostage when these checklists were introduced. However, the institution of these formal structured checklists dramatically reduced the incidence of blood stream infections to almost zero. Indeed, checklists managed variance between practitioners and institutions, and established clear benchmarks for overall perioperative anesthesia safety and quality, making me a believer.1,2 It no longer mattered what you or I as an individual wanted to do…you had to follow the checklist. Along the way, we lost a lot of our individuality and freedom on how we practiced. And this freedom and improvisation is why many of us went into medicine in the first place. I wonder what you think about all of this? After reading today’s PAAD please send me your thoughts for a Friday Reader Response.
In today’s PAAD, Saha and Segal3 demonstrated how a structured intraoperative handoff tool between anesthesia providers during ADULT non-cardiac surgery of at least 1 hour anesthesia duration significantly reduced the risk of adverse events. This idea of an intraoperative handoff tool or checklist has been around for quite a while, at least a decade or more, but to my knowledge this is the first quality improvement initiative/study to prove its value. By porting the checklist to the EMR (Epic) the use of the checklist took off and according to the authors is sustainable. I’ve asked 2 of my colleagues, Drs. Jamie McElrath Schwartz and Eugenie (“Genie”) Heitmiller, who have long thought about and studied the use of checklists perioperatively and in the PICU to assist. But first a word from Dr. Glaucomflecken. Myron Yaster MD
Original article
Saha AK, Segal S. A Quality Improvement Initiative to Reduce Adverse Effects of Transitions of Anesthesia Care on Postoperative Outcomes: A Retrospective Cohort Study. Anesthesiology. 2024 Mar 1;140(3):387-398. doi: 10.1097/ALN.0000000000004839. PMID: 37976442.
Every anesthesiologist is taught early: Never say no to the offer of a break! As much a part of our practice and culture as the stethoscope around our necks, breaks are important because they help us avoid provider fatigue, provide bathroom breaks, time for nursing mothers to pump breast milk, and/or offer the presence of a fresh perspective to an ongoing case. And yet despite its ubiquity, “critical details may be lost during the transition and transfer of care which many people believe may contribute to adverse patient outcomes.”3 Saha and Segal hypothesized that intraoperative handovers of anesthesia care with a structured intraoperative handover tool incorporated in the electronic medical record would be associated with decreased adverse patient outcomes.
In this retrospective study from a single institution, the Wake Forest University School of Medicine, Winston-Salem, North Carolina, Saha and Segal studied 121,077 cases, 40.4% of which had an intraoperative handover. Their “primary outcome was a composite of all-cause mortality in the 30 days after surgery and occurrence of postoperative morbidity (“morbidity composite”), which includes Centers for Medicare & Medicaid Services (Baltimore, Maryland) Patient Safety Indicator 90 (PSI-90) and Hospital Acquired Conditions and other in-hospital morbidities. Secondary and exploratory outcomes included morbidity composite, 30-day all-cause mortality, 1-yr all-cause mortality, safety event (activation of the rapid response team or cardiac arrest team), unplanned intensive care unit admission, hospital readmission within 30 days after discharge, remaining intubated at case end, postoperative reintubation, length of stay index more than 1 (indicating actual length of stay higher than predicted length of stay), postoperative visual or verbal analog pain score greater than 5 of 10, and emergency department visit within 30 days after discharge.”3
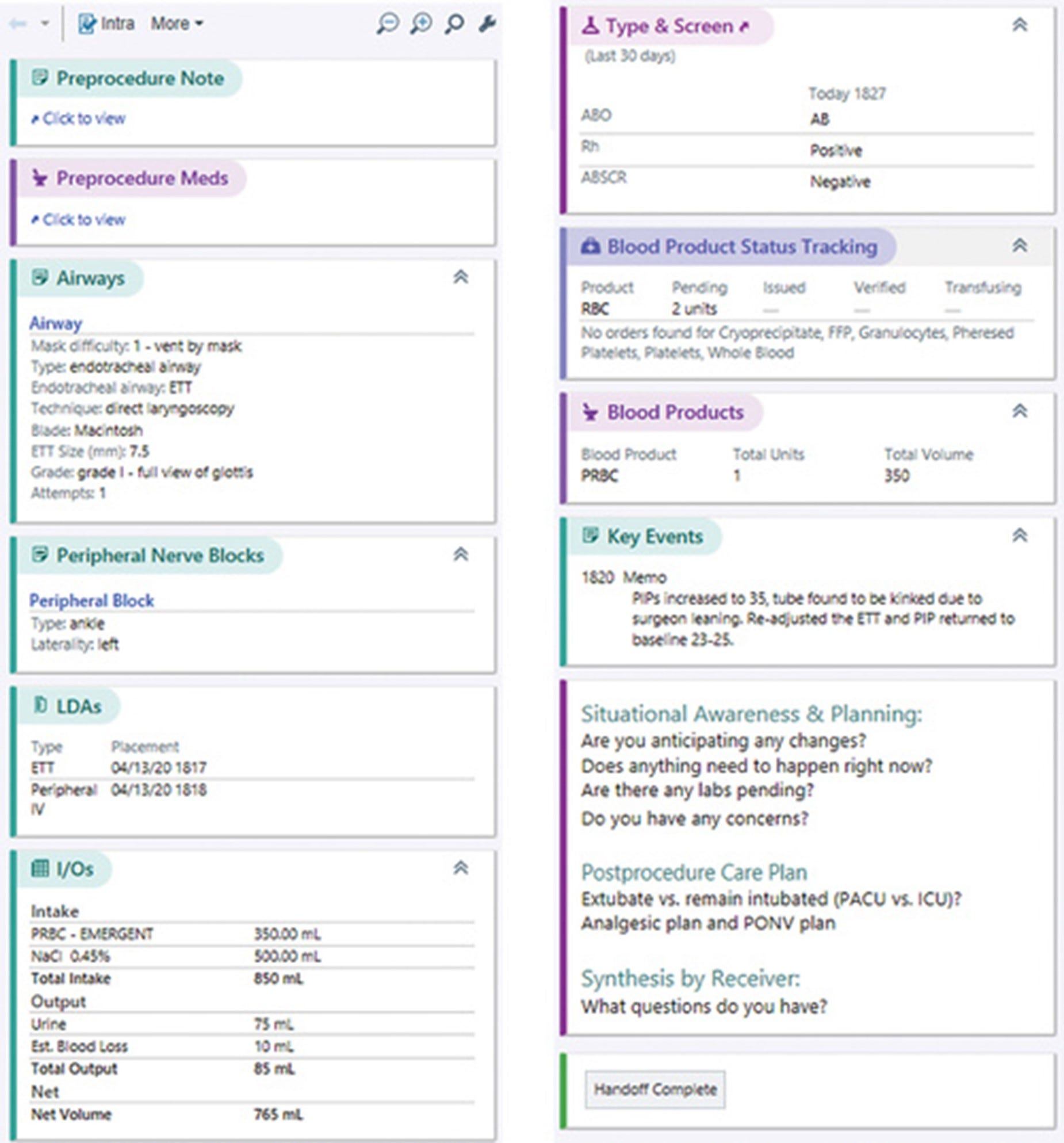
Based on preliminary findings, the authors instituted a quality improvement initiative “to promote the use of a structured tool built into the Epic electronic medical record during all permanent handovers of care, with documentation in the record.”3 “The handover tool (see in figure below) includes a case summary including visibility of the preoperative note, preoperative medications, airway management, regional anesthetic blocks, intravenous and arterial catheter details, current fluid totals and estimated blood loss, blood availability, free text “quick notes,” anesthesia events and times, and prompts to discuss anticipated changes, immediate patient needs, provider concerns, and postoperative plans including extubation, patient destination, and plans for management of postoperative analgesia and postoperative nausea and vomiting. In addition, the graphical display shows all medications administered with running case totals and patient hemodynamics. An icon on the anesthesia record illustrates the time of the current and any previous handovers, and the presence of such an event was counted as use of the tool.”3

OK, what did they find? Let’s cut to the chase. It worked! “The authors found that intraoperative handovers significantly increased the risk of adverse events during noncardiac surgery. However, the use of a structured handover tool that was developed by the authors during a quality improvement initiative significantly reduced the risk during intraoperative handovers.”3
Are there problems with this study? Absolutely! As the authors themselves explain: “First, the retrospective nature of the study and the temporal correlation of structured handovers with improving outcomes is not a demonstration of causality. Only a randomized trial, most likely in a block design by institution rather than at the individual provider level (to avoid learning contamination bias), could support a causal mechanism. Second, our observed decline in relative risk was modest, although sustained over2 years. A longer-term follow-up, demonstrating persistence of the salutary effect over time, would strengthen our conclusion. Further, we utilized a composite outcome, and it is possible that results for individual components may be fragile. Third, our study, like most in this field, is a single-institution investigation. It is likely that practice style, culture of safety, and staffing and relief models could influence the effects of handovers and structured tools. In particular, the overall frequency of handovers should be investigated as an independent predictor of their effect on outcomes. Validation of our results in other institutions would be helpful in this regard. Fourth, learning contamination bias could diminish the effect of a structured tool over time if clinicians learned to perform a better handover during its original introduction, even if it were subsequently omitted. Moreover, we made no attempt to evaluate handover quality or verify that the tool was actually used appropriately, but handovers in which the tool was activated but not utilized would tend to bias the results to the null, strengthening our conclusions. Finally, we did not differentiate the risks associated between handovers involving resident physicians versus CRNAs, nor did we study a dose–response relationship by analyzing the effect of number of handovers.“3
We think the time is long overdue to replicate this study in pediatric anesthesia and we are ideally suited to do this through our professional Societies and with the informatics knowledge of many of our readers and members. We need to marshal the data contained in our EMRs through programs like AdaptX. Further, in a well-designed study we can answer many of the questions left unanswered in the study by Saha and Segal.
What do you think? What do you think about checklists in general and loss of improvisation and jazz in our practice? Send your thoughts to Myron who will post in a Friday reader response.
References
1. McKee C, Berkowitz I, Cosgrove SE, et al. Reduction of catheter-associated bloodstream infections in pediatric patients: experimentation and reality. PediatrCrit Care Med 2008;9(1):40-46.
2. Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Critical care medicine 2004;32(10):2014-20. (In eng). DOI: 10.1097/01.ccm.0000142399.70913.2f.
3. Saha AK, Segal S. A Quality Improvement Initiative to Reduce Adverse Effects of Transitions of Anesthesia Care on Postoperative Outcomes: A Retrospective Cohort Study. Anesthesiology 2024;140(3):387-398. (In eng). DOI: 10.1097/aln.0000000000004839.