
Challenge-Response Aviation Checklists: How Process and Mindset Drive Safe Practice
David Liston MD MPH, Daniel Low MD MBBS, Lynn Martin, MD MBA

Original Review Article
Low DK, Reed MA, Geiduschek JM, Martin LD: Striving for a zero-error patient surgical journey through adoption of aviation-style challenge and response flow checklists: a quality improvement project. Pediatr Anesth. 2013;23:571-578. doi: 10.1016/j.jclinane.2017.12.008. PMID: 29505959
Checklists have become an essential part of OR safety. However, not all checklists offer the same level of utility. Some are far superior. Challenge-response checklists are a format and style borrowed from aviation. Several key points differentiate them from commonly used checklists in healthcare, the majority of which are in a ‘read-do’ format. The process is scripted with predetermined team members; one reading the challenge and another answering with a response – this ‘activates’ the whole team and creates a shared mental model that the patient / equipment / team are all configured correctly for the next part of the surgical journey.
Every challenge is deliberately brief (often simplified to one word) and specific. Every response is also very specific (scripted) and where possible include physical gestures (pointing, touching, calling out) to demonstrate task completion. Thus any team member, even those not directly involved in the challenge or response, can stop the process to either ask for clarification or point out if a response is incorrect.
While challenge-response checklists have been standard of care in both our main OR and ambulatory surgery center at Seattle Children’s Hospital for over 10 years, this was not the original format of our regional anesthesia checklist until more recently. Thus, we wanted to share our experience over the past 16 years as we believe the process of learning from the ‘never event’ of wrong-sided blocks resulted in the very robust regional anesthesia checklist that we use today.
In 2008, a wrong sided block occurred in a patient with two bilateral lower extremity procedures planned – one side major and a second side minor. Unclear surgical side marking led to the peripheral nerve block being placed on the wrong (minor) surgical side. The error was recognized at surgical time out. A Root Cause Analysis (RCA) was performed with the following corrective actions: 1) conversations between attending surgeon and attending anesthesiologist to occur PRIOR to the regional block, 2) surgical time out to occur BEFORE regional block procedure, 3) surgical site mark and consent define laterality (laterality removed from surgical schedule), 4) minimum of three team members present when performing the regional time out (attending anesthesiologist, OR circulating RN, anesthesia fellow/resident/tech) .
These corrective actions appeared to address, in depth, the cause of the wrong sided block. However, not determining the true root cause of the problem led to another event 6 years later. In 2014, a wrong sided block occurred in a patient having 2 surgical procedures, one lateral and one midline. The surgeon marked the wrong side (confirmed by parents). Subsequently the peripheral nerve block was placed on the wrong side. The clinic note and consent stated the correct side. The error was recognized at surgical timeout. An RCA was performed with the following corrective actions: 1) regional time out to occur before regional block procedure, 2) anesthesiologist reviews BOTH consent and site mark, 3) regional anesthesia checklist created to support the process.
Once again, we felt confident after these further corrective measures that the cause had been addressed. Then, in 2021 a wrong sided block occurred in a patient when a delay and distraction occurred between the regional time out and block placement with the surgical side covered with a blanket in the interim period. Time pressure was also felt to be a contributing factor. An RCA was performed with the following corrective actions: 1) block prep in advance of timeout, 2) timeout done IMMEDIATELY prior to start of block, 3) time out changed to scripted Challenge-Response format, 4) no parallel work during block timeout or placement, 5) marking of block site by anesthesiologist.
These changes were supported by a meta-analysis published in the Journal of Clinical Anesthesia in 2018 that listed 3 procedural steps to help prevent wrong sided blocks:
1) Verify nerve-block procedure using multiple sources of information.
2) Identify the nerve-block procedure with a visible mark.
3) Perform time-outs immediately prior to injection or installation of anesthetics.
After multiple wrong sided block events, we believe a true root cause was finally determined by continuing to ask the “5 whys”. It is important for each hospital to have a preoccupation with failure and to always be looking for iterative improvements. Those that make mistakes should be neither blamed nor punished, instead look at the system. The focus for improvement after such an event should be on systems / process / workflow issues, not on individual practitioner competency issues.
As noted in the article by Fould, when advocating for aviation checklists “Recognize that humans, by our very nature, make mistakes. Our personalities are composed of the cognitive, the emotional, and the behavioral. Three chances to get things right. Three chances to get things wrong. We get in a hurry, we get distracted, we get complacent, or we get tired, and we miss something… I don’t think you can train the human out of a standard pilot. But you can add a layer of safety to account for the human factors at play.” In our final iteration, we changed our standard checklist format to the aforementioned aviation style challenge and response checklist – clearly defining roles (RN issues challenge / anesthesiologist performing the block responds).
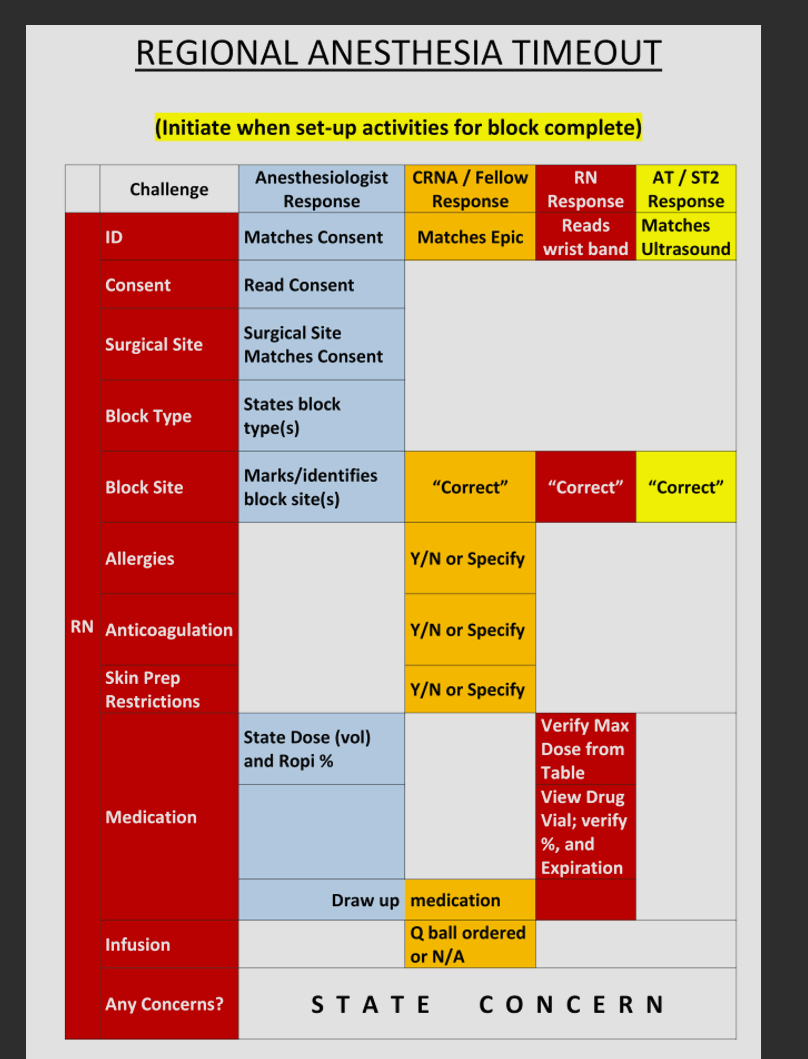
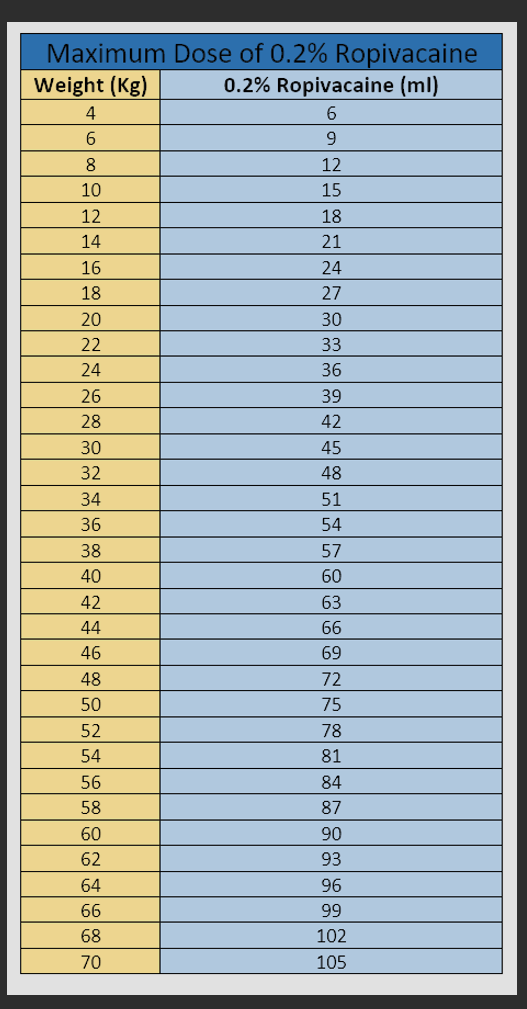
We also incorporated drawing up medications ‘just in time’ immediately prior to the block and use independent confirmation via a reference card to verify correct medication and ceiling max dose.
Reflecting on our experience, we firmly believe that well-structured challenge-response checklists in conjunction with well-trained teams and a culture of iterative process improvement did lead to improvements in patient safety. The common enemy is now team complacency. Be safe out there!
Send your thoughts and comments to Myron who will post in a Friday reader respojnse.
References
1. Fould, D. Challenge response: should medical crewmembers help with pre-takeoff checks? 11 Dec. 2017, https://verticalmag.com/features/challenge-response-medical-crewmembers-help-pre-takeoff-checks/ Accessed 5 Apr. 2024.
2. Deutsch ES, Yonash RA, Martin DE, Atkins JH, Arnold TV, Hunt CM: Wrong-site nerve blocks: A systematic literature review to guide principles for prevention. J Clin Anesth. 2018;46:101-111.doi: 10.1016/j.jclinane.2017.12.008. PMID: 29505959