
Cerebral autoregulation monitoring: an approach to individualized blood pressure management to protect the brain during and after heart surgery?
Ken M. Brady, MD and R. Blaine Easley, MD

Over the past couple of months, we’ve discussed both the definitions and treatment of hypotension in the perioperative anesthetic management of children. To be honest, it’s pretty amazing to me that much of this remains unknown and that our reality and interpretation are often out of synch (Plato’s cave). Drs, Ken Brady, Blaine Easley, and Jenny Lee are THE experts and leaders in studying this. Jenny was out of band width and couldn’t help in writing the PAAD, but Ken and Blaine could, and the following, hopefully, will open your eyes to an entirely different way of thinking about the lower limits of autoregulation and blood flow to the brain. Some of this has previously been presented at SPA and CCAS meetings and remains unknown to many of you. One of the great things about Ken, Blaine, and Jenny is that they can take a complex and mathematically complex subject (Fourier analysis anyone?) and make it understandable to the mathematically challenged. A revisit of these issue would be very timely and I’m hoping will be a subject of discussion and education at a future SPA annual meeting.
Before launching today’s PAAD, I’ve got to acknowledge that on a very personal level I am just so proud of Ken, Blaine and Jenny. All were my fellows and trained at Johns Hopkins in a magical time. Their careers and discoveries are a real testament to that program and to their grit and determination and what one can accomplish as an academic pediatric anesthesiologist. Ken is currently the Division Head, Cardiac Anesthesia; Section Head, Regenstein Cardiac Intensive Care Unit; Gracias Family Professor in Cardiac Critical Care. He is a Professor of Anesthesiology and Pediatrics, Northwestern University Feinberg School of Medicine, Lurie Children’s Hospital. Blaine is currently the Division Chief, Critical Care Anesthesiology at Texas Children’s Hospital and Professor of Anesthesiology and Pediatrics, Baylor College of Medicine. Jenny is a Professor of Anesthesiology/Critical Care Medicine and Pediatrics and the Senior Associate Dean for the Office of Women in Science and Medicine at the Johns Hopkins University and Medical School. Many of you know Jenny from her leadership role in SPA’s Women’s Empowerment and Leadership Initiative (WELI). Myron Yaster MD
Original article1
Brady KM, Hudson A, Hood R, DeCaria B, Lewis C, Hogue CW. Personalizing the Definition of Hypotension to Protect the Brain. Anesthesiology. 2020 Jan;132(1):170-179. PMID: 31644437
If you care for critically-ill children, you manage hypotension. You make decisions about volume expansion, inotropy and vasoactive medications based on blood pressure thresholds that you believe safe to perfuse your patient’s brain. The threshold you choose is not evidence-based because our specialty has failed to delineate such a threshold. Even if you target normative values of blood pressure by age or weight, how do these targets apply to your patient and their clinical scenario? Belief and truth are topics best left to theologians and philosophers. Evidence is the substance of hubris, and we are not so naïve as to think that we have enough to guide difficult clinical choices. Regarding this fundamental choice (how much blood pressure is enough?) made regularly by every pediatric anesthesiologist and intensivist, we are in the dark, chained to Plato’s cave.
Studies conducted over the past decade have highlighted clinical variability in definitions of normotension and interventions for hypotension in infants and children undergoing anesthesia. Two salient examples of poor adherence to blood pressure standards during anesthesia are 1) the McCann et al.2 case series of neonates developing encephalopathy, and 2) the CORE (Center for Outcomes Research and Evaluation) sub-analysis of the GAS study.2, 3 Both publications report neonates and infants undergoing routine anesthetics for various surgical procedures, and their findings propose an association between poor neurologic outcomes and blood pressure management.
However, it has long been recognized that infants and children with congenital heart disease undergoing complex repairs on cardiopulmonary bypass have a much higher risk for developing stroke, seizure, brain injury and poor neurodevelopmental outcomes with multiple modifiable and non-modifiable risk-factors. The watershed white matter injury seen in these patients is highly suggestive of hypotensive brain injury. The survival of neonates with critical heart disease, especially shunted patients, depends on afterload reduction and balanced systemic and pulmonary circulations. While the strategy for afterload reduction has been debated, the need for afterload reduction is accepted.4, 5 However, it is also accepted that this hypotensive strategy comes with a risk of watershed brain injury. When your patient requires a low arterial blood pressure, how low is safe? You do not know the answer to this question because our specialty has not answered it. The autoregulation monitor attempts to fill this knowledge gap.
The autoregulation monitor was a pivot away from measuring cerebral blood flow, which is possible to do but unhelpful clinically. Rather than target specific flow rates, the autoregulation monitor seeks to delineate the blood pressure range that allows cerebral vasoreactivity to regulate flow. For instance, the autoregulation monitor can delineate the “optimal” blood pressure which is associated with the most robust vessel reactivity and the best outcomes after traumatic brain injury MAPopt. Alternatively, the autoregulation monitor can delineate the lower limit of autoregulation, the blood pressure at which vessel reactivity fails (LLA). The LLA serves as a logical boundary of blood pressure for patients who need afterload reduction. Commutative logic suggests that blood pressures associated with vessel reactivity, above the lower limit of autoregulation, will be associated with flow that is regulated and therefore safe.
The recent study from Zipfel et al,6 done at the University of Tubingen, Germany deployed near infrared spectroscopy-based autoregulation monitoring to identify MAPopt and LLA for 16 hours following cardiac surgery. MAPopt and LLA were compared to institutional guidelines used at Tubingen for blood pressure by age. Using a prospective, observational study design, infants undergoing CPB (cardiopulmonary bypass) were provided routine bedside care in the postop period while autoregulation monitoring was recorded. Management followed institutional practice with therapeutic goal of MAP > 33 mmHg for subjects < 6 months, and MAP > 43 mmHg for subjects > 6 months. Thirty-six infants (20% cyanotic lesions) with an average age of 4.1 months and weight of 5.2kg were enrolled. For 50% of subjects, the measured LLA was higher than the institutional standard for acceptable MAP (mean LLA of 48.8 + 8.3 mmHg; range 29 to 68.5). This resulted in 1/3 of all monitored time with blood pressure that was too low to support autoregulation. Suggesting the potential for long periods of time with sub-optimal blood flow to the brain.
Autoregulation of cerebral blood flow is not a new concept, but the real-time ability to monitor autoregulation developed in the last 25 years synchronous with advancements in computing power. Most anesthesiologists can remember the number 50 mmHg as a lower limit of autoregulation cited in textbooks (Figure 1).7,14 This comes from Lassen’s curve, a compilation of cerebral blood flow studies done by Nils Lassen in 1959. That curve is shaped at the lower limit exclusively by data from pre-eclamptic patients. Ironically, the study was entitled “cerebral blood flow in man.” How applicable is that number to your patient? In 1996, Marek Czosnyka and the neurosurgical physics research group at Cambridge published a method to analyze the phasic relationship (by serial correlation) of intracranial and arterial blood pressure slow waves.
The Cambridge method was influenced by observations of intracranial pressure waves by Nils Lundberg in the 1960’s and his assertion that the slow “B” waves represented vasoreactivity and autoregulation. The algorithm developed by the Cambridge group is called the Pressure Reactivity Index and is the most widely studied method in the field.8 Does autoregulation monitoring work? A landmark study by the Cambridge group demonstrated that the pressure reactivity index could identify optimal cerebral perfusion pressure in adults with traumatic brain injury that was related to both neurologic outcome and survival.9, 10 Based on these findings, autoregulation monitoring was introduced as an option in published TBI guidelines starting in 2004.11 Lessons learned from the Cambridge method have since been applied to non-invasive modalities such as trans-cranial Doppler and near infrared spectroscopy. These have been validated to delineate LLA accurately, and with similar receiver operator characteristics to the invasive method.
Can non-invasive cerebral autoregulation monitoring guide blood pressure management in high-risk populations without neurosurgical intervention? Non-invasive versions of the Cambridge technique have been applied to adult and pediatric populations using both trans-cranial Doppler and near-infrared spectroscopy. Most notably, there has been a prospective randomized trial of autoregulation guided blood pressure management in adults undergoing coronary artery bypass surgery with cardiopulmonary bypass. Brown et al.12 found that targeting BP management using autoregulation monitoring resulted in improved post-op cognitive test scoring and reduced incidence of delirium. Hogue et al.13 found no significant difference in postop brain imaging (probably because thromboembolic lesions are not expected to be impacted by blood pressure), but found reduced rates of acute kidney injury, shorter length of ICU and hospital stay and lower rates of neurocognitive dysfunction in the individualized BP guided group.
After two decades of investigating these autoregulation monitoring techniques, we seem to have raised as many questions as we have answered: What is the best technique to use when measuring autoregulation? A myriad of techniques are reported in the literature with variations in the modality used to interrogate the brain and the signal processing techniques used to analyze the resultant waveforms. How fast does the monitor have to report results to be useful? How much inaccuracy can be tolerated in the monitor? Speed and accuracy are inversely proportional in autoregulation monitoring. How much green light do we have to use this technology on patients? The best data supports use in adults undergoing cardiac surgery, but this is not the same clinical scenario as a neonate undergoing cardiac surgery. Consider the paucity of evidence supporting clinical monitors we currently use: The pulse oximeter has never been shown to improve outcome for surgery, but it has become a de facto standard of care based on our collective experience with it. When the pulse oximeter was first introduced, how many patients with ARDS suffered ventilator-associated lung injury as practitioners chased 100% oxyhemoglobin saturation? Who is most likely to be hurt by rolling out the autoregulation monitor for clinical use? Afterload reduction after neonatal cardiac surgery is fundamental to the survival rates we currently enjoy. What will the autoregulation monitor do to this practice, and will it be safe? Do we target blood pressure that optimizes autoregulation (as proposed by the Tubingen study) or do we target blood pressure above the lower limit of autoregulation (as in the Hogue study)?
Commercial autoregulation monitors are beginning to appear in European markets (Raumedic, https://www.raumedic.com/us/application-areas/neuromonitoring/neuro-icu/neurosmart). Autoregulation monitoring can be done with bedside computing using the Cambridge software (ICM+, https://icmplus.neurosurg.cam.ac.uk/) and home-grown physiologic waveform monitoring systems also have the ability if programmed correctly. In the United States two FDA-cleared platforms have autoregulation monitoring features for research use only: the Moberg and Sickbay systems (https://www.moberg.com/, https://michealthcare.com/sickbay/). As these devices gain traction, and clinicians have more experience with them, the window to conduct further randomized trials will close. As with every other monitor we use clinically, the autoregulation monitor will either be perceived useful or not, and this will determine how they are used by the average practitioner.
Figure
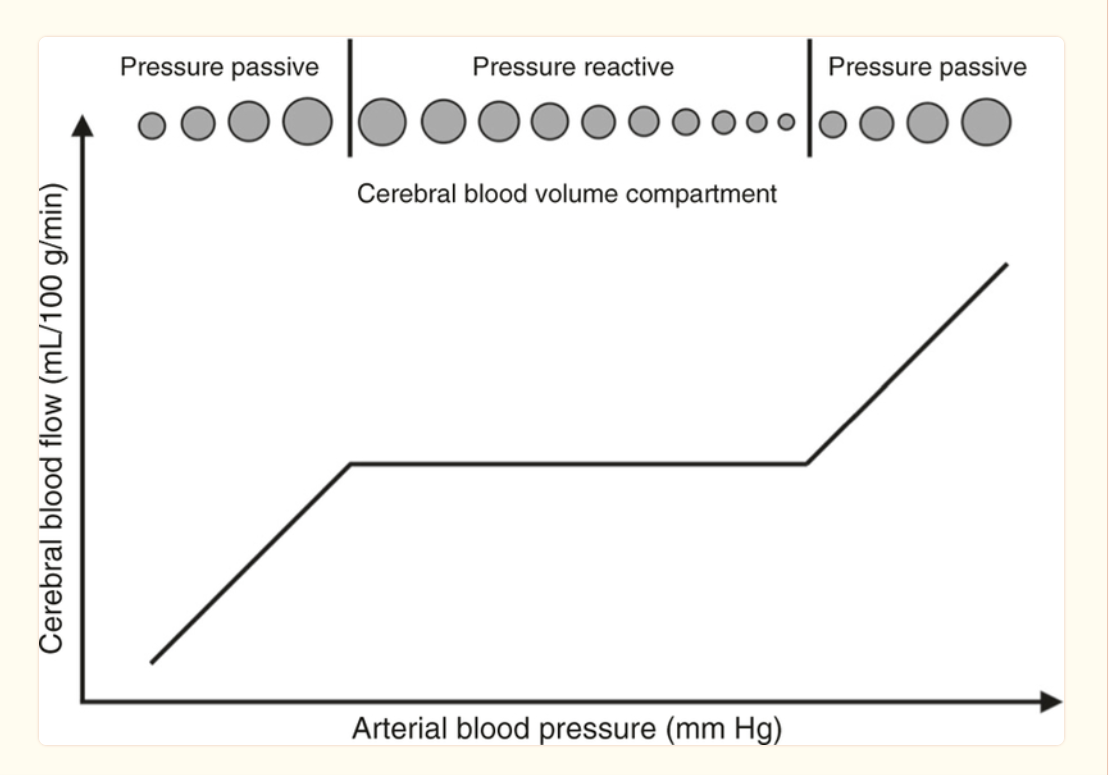
Schematic of “Lassen’s Curve” with cerebral blood flow over changes in blood pressure. Note the stability (no change in blood flow) between the upper and lower limit of autoregulation. Also note the schematic of blood vessel/blood volume changes relative to the change in blood pressure to maintain constant blood flow in arterial blood pressure that supports intact autoregulation.14
References
1. Brady KM, Hudson A, Hood R, DeCaria B, Lewis C, Hogue CW. Personalizing the Definition of Hypotension to Protect the Brain. Anesthesiology. Jan 2020;132(1):170-179. doi:10.1097/aln.0000000000003005
2. McCann ME, Schouten AN, Dobija N, et al. Infantile postoperative encephalopathy: perioperative factors as a cause for concern. Pediatrics. Mar 2014;133(3):e751-7. doi:10.1542/peds.2012-0973
3. McCann ME, Withington DE, Arnup SJ, et al. Differences in Blood Pressure in Infants After General Anesthesia Compared to Awake Regional Anesthesia (GAS Study-A Prospective Randomized Trial). Anesthesia and analgesia. Sep 2017;125(3):837-845. doi:10.1213/ane.0000000000001870
4. Stuth E. Phenoxybenzamine is indicated in treatment of hypoplastic left heart syndrome: pro. Anesthesia and analgesia. Aug 2007;105(2):307-9. doi:10.1213/01.ane.0000271915.56275.0c
5. DiNardo JA. Phenoxybenzamine is indicated in treatment of hypoplastic left heart syndrome: con. Anesthesia and analgesia. Aug 2007;105(2):310-1. doi:10.1213/01.ane.0000278952.27339.74
6. Zipfel J, Wikidal B, Schwaneberg B, et al. Identifying the optimal blood pressure for cerebral autoregulation in infants after cardiac surgery by monitoring cerebrovascular reactivity-A pilot study. Paediatric anaesthesia. Dec 2022;32(12):1320-1329. doi:10.1111/pan.14555
7. Lee JK. Cerebral perfusion pressure: how low can we go? Paediatric anaesthesia. Jul 2014;24(7):647-8. doi:10.1111/pan.12404
8. Rhondali O, Juhel S, Mathews S, et al. Impact of sevoflurane anesthesia on brain oxygenation in children younger than 2 years. Paediatric anaesthesia. Jul 2014;24(7):734-40. doi:10.1111/pan.12397
9. Aries MJ, Czosnyka M, Budohoski KP, et al. Continuous determination of optimal cerebral perfusion pressure in traumatic brain injury. Critical care medicine. Aug 2012;40(8):2456-63. doi:10.1097/CCM.0b013e3182514eb6
10. Steiner LA, Czosnyka M, Piechnik SK, et al. Continuous monitoring of cerebrovascular pressure reactivity allows determination of optimal cerebral perfusion pressure in patients with traumatic brain injury. Critical care medicine. Apr 2002;30(4):733-8. doi:10.1097/00003246-200204000-00002
11. Kochanek PM, Tasker RC, Carney N, et al. Guidelines for the Management of Pediatric Severe Traumatic Brain Injury, Third Edition: Update of the Brain Trauma Foundation Guidelines. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies. Mar 2019;20(3S Suppl 1):S1-s82. doi:10.1097/pcc.0000000000001735
12. Brown CHt, Neufeld KJ, Tian J, et al. Effect of Targeting Mean Arterial Pressure During Cardiopulmonary Bypass by Monitoring Cerebral Autoregulation on Postsurgical Delirium Among Older Patients: A Nested Randomized Clinical Trial. JAMA surgery. Sep 1 2019;154(9):819-826. doi:10.1001/jamasurg.2019.1163
13. Hogue CW, Brown CHt, Hori D, et al. Personalized Blood Pressure Management During Cardiac Surgery With Cerebral Autoregulation Monitoring: A Randomized Trial. Semin Thorac Cardiovasc Surg. Summer 2021;33(2):429-438. doi:10.1053/j.semtcvs.2020.09.032
14. Rhee CJ, da Costa CS, Austin T, Brady KM, Czosnyka M, Lee JK. Neonatal cerebrovascular autoregulation. Pediatr Res. Nov 2018;84(5):602-610. doi:10.1038/s41390-018-0141-6