
Blood Transfusion
Myron Yaster MD, Genie Heitmiller MD, Allison Kinder Ross MD, and Susan M. Goobie MD FRCPC

The June 2025 issue of the ASA Monitor has several terrific articles devoted to blood transfusion. Managing active bleeding is an essential part of our practice, and if you are like me, just thinking about the coagulation cascade (and the Krebbs cycle) brings back medical school nightmares, cold sweats and the desire to open the window and scream into the night! Nevertheless, how to use and dose antifibrinolytics like tranexamic acid (TXA) and targeted coagulation products like fibrinogen complex concentrates when patients are bleeding in the ORs and ICUs always brought on the imposter syndrome in me. I knew I had to be an expert but never really felt like I was. Because of this I’ve asked three members of the PAAD executive council, Drs. Genie Heitmiller, Allison Kinder Ross, and Susan Goobie to assist. In today’s PAAD we are going to concentrate on the articles in this issue that deal with how to manage acute bleeding and coagulopathy in the ORs and ICUs.1 I am also including an Open Mind article by Dudaryk et al. from the June 2025 issue of Anesthesia and Analgesia. In tomorrow’s and Monday’s PAAD, we will discuss the unique considerations of patient blood management in pediatrics.
Finally, I used to joke that blood banks and their approach to blood products was similar to how grocery stores sell milk and chicken. When you go to the grocery store you want milk that is the freshest and will last longest in your fridge. On the other hand, the grocery store wants you to buy its oldest milk before they reach their expiration date. Thus, they move those containers to the front of the refrigerator case. Blood banks are similar. They want you to transfuse their oldest blood and don’t want to provide you with their freshest blood for the same reasons…they don’t want their blood to expire. And the blood bank wants you to use blood products, like red blood cells, plasma, and platelets rather than whole blood, just like the supermarket wants you to buy chicken parts rather than a whole chicken. Cynically, the grocery stores can make a lot more money on the parts than on the whole, but that’s not the only reason for using component blood products. Component blood therapy allows the clinician to administer only what the patient needs, reduces risk of potential adverse reactions, allows for longer storage periods, and potentially reduces blood product wastage. And yet, as we will see, there may be advantages to fresh whole blood and a shift is occurring to consider the use of fresh whole blood in actively bleeding adult and pediatric trauma patients, neonates, and in pediatric cardiac surgery patients. Finally, in today’s PAAD, I’m going to review basic information and would urge all of you in teaching institutions to take advantage of today’s PAAD while working with students in the OR today. Test your own and their knowledge! Myron Yaster MD
Original article
Nicholas, Joshua MD, FRCPC; Panigrahi, Anil K. MD, PhD, FASA. Advances in Transfusion Medicine. ASA Monitor 89(6):p 13-14, June 2025. | DOI: 10.1097/01.ASM.0001118144.06446.c9
The Open Mind
Dudaryk, R. , Meizoso, J. & Schreiber, M. (2025). The New Old Solution: Whole Blood for Nontraumatic Hemorrhage. Anesthesia & Analgesia, 140 (6), 1359-1362. doi: 10.1213/ANE.0000000000007217.
You are managing a trauma patient who is actively bleeding. You send appropriate labs and need to resuscitate and transfuse. You know that excessive use of isotonic balanced salt solutions makes things worse. What are your options?
Traditionally, hemodynamic and hemostatic resuscitation for trauma and critical massive hemorrhage in the OR and ICU was to primarily administer crystalloids and red blood cells. From lessons learned in military combat, hemostatic resuscitation has evolved to a balanced approach with the transfusion of blood components in a fixed ratio of 1:1:1 or 2:1:1 red blood cells, plasma, and platelets (and also including a fibrinogen source such as cryoprecipitate or fibrinogen concentrate) which more closely recreates the composition of whole blood. “This novel approach has been instrumental in mitigating the early stages of trauma-induced coagulopathy by promptly replenishing coagulation factors and platelets. Moreover, it has played a critical role in reducing the incidence of dilutional coagulopathy, a phenomenon prevalent with crystalloid-based resuscitation.”2
It should be noted that for all hospitals treating bleeding children it is recommended (and required by the American College of Surgeons Children’s Surgery Verification) to have a goal-directed Massive Hemorrhage Protocol (MHP) or Massive Transfusion Protocol (MTP) to standardize care. These protocols should be based on age- or weight-appropriate guidelines, and evidence- or consensus-based transfusion algorithms. They facilitate timely recognition and treatment of hemorrhagic shock, employing damage control resuscitation principles effectively to stop bleeding and prevent and manage coagulopathy (and may include viscoelastic testing), while minimizing morbidity and mortality associated with or potentially worsened by under- or over-transfusion.
Using component therapy to simulate whole blood when treating massive hemorrhage perhaps is not optimal. Why not simply use whole blood? “Interestingly, whole blood was the mainstay of hemorrhagic shock resuscitation from the 19th century until the Vietnam War in civilian practice. The shift to component therapy-based resuscitation strategies occurred not because of demonstrated superiority or equivalence but due to advances in fractionation. These advances allowed for longer shelf-life of blood components, making them more readily available for remote conflicts—a change quickly embraced by the US military.”2 Dudaryk et al. also point out that fractionating blood is very profitable for blood banks but this “may shift with the growing preference and demand for whole blood.”2
Whole Blood
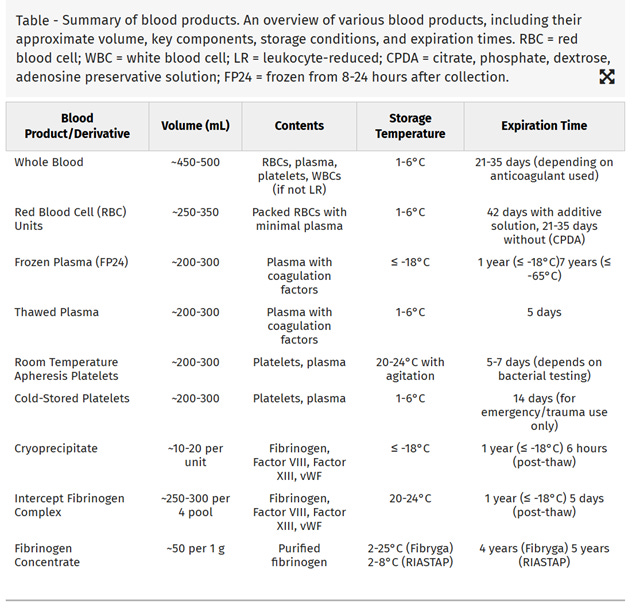
“Given reported improved outcomes observed with balanced ratio transfusions (PRBC:FFP:Platelets 1:1:1 or 2:1:1), there has been renewed interest in using whole blood during trauma and massive hemorrhage resuscitation. Whole blood delivers all components rapidly in a single product. Cold storage has emerged as a strategy to address logistical limitations of using warm fresh whole blood in civilian populations. The type of whole blood carried by most civilian centers is blood group O with low isohemagglutinin (anti-A, anti-B antibody) titers, referred to as low-titer group O whole blood (LTOWB). This product is FDA approved for storage at 1-6°C for 21 or 35 days depending on the preservative solution. There are several benefits attributed to the use of LTOWB. It can be used even when the blood type of the recipient is unknown, it contains fewer anticoagulants and additives than component products, which may improve their hemostatic profile and reduce hemodilution, and may have a beneficial effect on platelet function in hemorrhaging patients and decrease the risk of bacterial growth compared to platelet units stored at room temperature. ”1 But few pediatric trauma centers or hospitals have whole blood available for transfusion, even for massive transfusion, and most continue to use component blood transfusion therapy. Those that do have LTOWB often reserve it only for initial transfusion in adults, but this may change as the evidence strengthens for improved outcomes with LTOWB transfusion in children.
Platelets
“Room temperature platelet (RTP) storage has been the predominant component for decades because of its greater average yield and lifespan after infusion in nonbleeding patients compared with cold stored platelets (CSPs). RTP have the functional shelf life of just over three days and allow for bacterial contamination. On the other hand, CSP maintains adhesion and aggregation in vitro for up to three weeks of storage and does not risk bacterial infection. The FDA has recently released a guidance for industry regarding CSP, allowing a shelf life up to 14 days for the treatment of actively bleeding patients in contexts where RTPs are not available or use is not practical”1
Fibrinogen
Targeted prevention and early treatment of hypofibrinogenemia may have morbidity and mortality benefit. There are 2 concentrated sources of fibrinogen: Cryoprecipitate – the cold insoluble proteins derived from frozen plasma (factors V, VIII, XIII, fibrinogen, and fibronectin) and Fibrinogen concentrate (FC) – lyophilized powder derived from pooled human plasma.
“Barriers to treatment with cryoprecipitate are typically related to product preparation. Cryoprecipitate requires thawing from a frozen state and, without pathogen reduction technology, expires six hours after thawing. This makes it impractical to maintain a liquid inventory for acute bleeding without excessive waste. As a result of the need to thaw, the time from order to administration of cryoprecipitate can be upward of 60 to 210 minutes. The introduction of pathogen reduction technology for cryoprecipitate offers a means of addressing this challenge. In November 2020, the FDA granted approval for the manufacturing system to produce pathogen-reduced cryoprecipitated fibrinogen complex (Intercept Fibrinogen Complex, IFC, Cerus, Inc.). IFC has a post-thaw shelf life of five days, making it feasible to maintain as a liquid product for rapid treatment of hypofibrinogenemia. Implementation of this product for surgical patients has reduced turnaround time and waste at multiple institutions.”
Fibrinogen Concentrate (FC) has been used off-label in the United States and is the standard in European countries and Canada to treat the acquired hypofibrinogenemia during cardiac surgery. The potential advantages of FC including rapid reconstitution, greater dose predictability, viral inactivation during processing, and reduced transfusion-related adverse events. FC has been investigated and found to be as effective in the pediatric cardiac setting as an alternative to cryoprecipitate for managing bleeding and hypofibrinogenemia after cardiopulmonary bypass (CPB).3 FC is used outside the US to replace cryoprecipitate in MHPs. For example, it is incorporated into the Canadian Pediatric Massive Hemorrhage Protocol https://transfusionontario.org/en/category/massive-hemorrhage-protocol/toolkit-mhp/ .
These advances in the storage of platelets and cryoprecipitate will hopefully ease the problem of their typical short supply. Furthermore, the use of recombinant products such as FC offers a reliable and perhaps safer alternative; the main consideration hampering routine use is the cost in the US. And the risk of bacterial contamination with platelets is real. I (GH) recall watching the blood pressure drop every time I started infusing platelets on a patient (a baby after cardiopulmonary bypass), I sent the product back to the Blood Bank and learned that it was contaminated product.
What are you doing in your practice? Do you have a Massive Hemorrhage Protocol? Is whole blood readily available? Send your thoughts and comments to Myron who will post your responses in a Friday reader response.
References
1. Nicholas J, Panigrahi AK: Advances in Transfusion Medicine. ASA Monitor 2025; 89: 13–14
2. Dudaryk R, Meizoso JP, Schreiber MA: The New Old Solution: Whole Blood for Nontraumatic Hemorrhage. Anesthesia & Analgesia 2025; 140: 1359–1362
3. Downey LA, Andrews J, Hedlin H, Kamra K, McKenzie ED, Hanley FL, Williams GD, Guzzetta NA: Fibrinogen Concentrate as an Alternative to Cryoprecipitate in a Postcardiopulmonary Transfusion Algorithm in Infants Undergoing Cardiac Surgery: A Prospective Randomized Controlled Trial. Anesth Analg 2020; 130: 740–751