


Artificial Intelligence and live interpretation of Ultrasound images
Hannah Lonsdale MBChB, Ali Hassanpour MD, and Julia Gálvez Delgado MD

When I was first learning how to use ultrasound for both central line placement and peripheral neural blockade, I was simply terrible. Aside from learning how to hold the probe, I just couldn’t “see” the structures I was looking for. My good friend, Dr. Santhanam Suresh of Lurie Children’s Hospital and a pioneer in the use of ultrasound for peripheral nerve blocks, took me under his wing and taught me how to look beyond the black and white dots and lines and learn pattern recognition to identify structures. The example he used was to look for the arrow in the FEDEX logo. The arrow in the Fedex logo? What arrow? This logo is one that I’d seen every day for years and I had never seen an arrow! However, once I, or now you, see it, you can never see anything except the arrow when you see the logo…OK, Look closely at the Ex below at the end of the logo. Can you see it now?

Today’s PAAD by Dr. Julia Galvez of the University of Nebraska Medical Center/Children’s Hospital Omaha and the PAADs primary reviewer of all things IT asked her mentees Dr. Hannah Lonsdale of Vanderbilt Children’s Hospital and Dr. Ali Hassanpour to review these articles on how artificial intelligence is being used to “find the arrow in the FEDEx logo” when doing peripheral nerve blocks. As you will see AI is ideally suited for this task. Finally, I’d like to emphasize that this is a very rapidly changing and dynamic field of investigation. The author’s of today’s PAAD have more papers recently published and in the pipeline.1-3
Aritficial intelligence? What could go wrong? Myron Yaster MD
Original article
Bowness JS, El-Boghdadly K, Woodworth G, Noble JA, Higham H, Burckett-St Laurent D. Exploring the utility of assistive artificial intelligence for ultrasound scanning in regional anesthesia. Regional Anesthesia & Pain Medicine. 2022 Jun 1;47(6):375-9. PMID: 35091395
How much of your life is currently assisted by artificial intelligence? Not much? More than you think? Artificial intelligence (AI) gets us from A to B in our cars through GPS, helps us find information using online search engines and even keeps our credit cards safe from fraud by detecting unusual transaction activity, to name but a few applications. AI algorithms are being incorporated in devices and information systems platforms across medicine. As of October 2022, the US Food and Drug Administration (FDA) had approved a total of 178 medical devices incorporating AI algorithms. These devices span many disciplines of medicine and have a wide range of applications including physiologic monitoring and image analysis. Only four currently approved devices are intended for use in anesthesiology, but many more are in development. Machine learning (ML) is one branch of AI where specialist algorithms produce models that give computers the ability to perform human-like actions such as problem-solving, object and word recognition, inference of world states and decision-making by generating complex mathematical functions. ML models require training and validation on large datasets. Machine Vision (MV) refers to a subtype of machine learning where the data source is comprised of images. The image-heavy medical specialties such as radiology and pathology have been quick to develop, validate and implement clinical decision support applications based on MV technology, and there are multiple areas of ongoing study in anesthesia and pediatric anesthesia.4-6
Today’s PAAD is a prospective evaluation of a commercially developed MV device that is designed to assist in recognizing anatomic structures visualized with ultrasound for the planning of peripheral nerve blocks (PNBs). The device consists of an accessory screen that is connected to a standard ultrasound machine and applies an overlay identifying relevant anatomic structures such as nerves, blood vessels and muscles in real-time B-mode. The authors evaluated the device in a simulation experiment where experts and non-experts in ultrasound guided regional anesthesia performed anatomical scans on two healthy adult males with BMIs of 26 and 36. While no blocks or interventions were performed, each participant was asked to achieve an optimal block view for 9 common PNBs in the upper and lower extremities as well as the trunk. The following image is from the article.
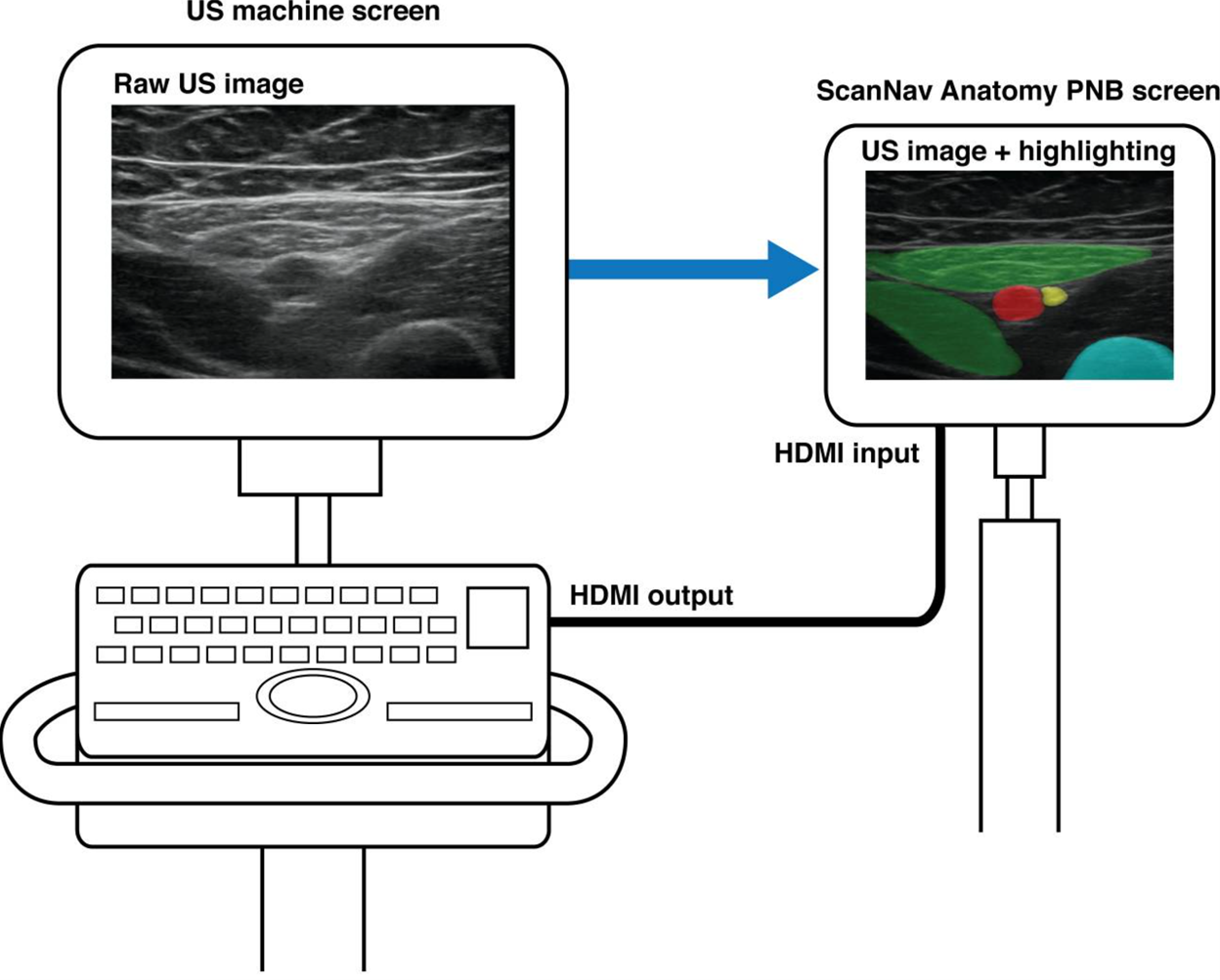
The following image is a screenshot from a promotional video and demonstrates how the software might be used in practice.

After every scan, participants were asked to complete a questionnaire based on their experience with the device. Questions included self-assessment of confidence in ability to scan and recognize anatomic structures, and usefulness in facilitation of training. In addition, every expert who performed scans and a further three remote experts were asked to report on a video of each scan, looking for any potential for increased risk of block failure or unwanted needle trauma to safety-critical structures. Many scanners (60% of non-experts, 50% of experts) agreed that the device could serve a useful future role in training and most (70%) reported that the device aided identification of key anatomical structures. The median confidence to perform the block was rated by experts at 10 out of 10 both with and without the device. There was no significant difference in the expert’s opinion on risk of harm during scans performed with or without using the new device. Of the negative feedback generated from experts, almost half (48%) originated from one participant. Over half of the non-expert negative feedback also originated from a single participant. Readers familiar with change management practice may recognize this type of behavior from individuals who are skeptical of new ideas and methods and are late adopters of practice changes.
Innovators and early adopters of new technology will be excited to learn when ScanNav might be available for clinical use. In October 2022 the device was granted FDA de novo (513(f)(2)) clearance for use in pre-procedural identification of structures. This use represents the lowest level of FDA risk classification and is therefore the “easiest” to achieve. The proposed use of ScanNav in pre-procedural scanning likely represents a “minimum viable product”- an offering with enough features to attract additional funding, and to attract support from early adopters and opinion leaders. In time we expect to see an expansion of capability that may include additional anatomical locations, suggested needle trajectories and support for intra-procedure use. Guidance for probe positioning would be a further useful addition.
Regulatory agencies including the US FDA are developing and refining the regulatory procedures that are applied to the evaluation of AI-enabled medical devices, most of which are found in radiology and cardiology. Other similar systems are also in development, including Nerveblox (Smart Alfa Teknoloji), which also applies a color overlay to anatomical structures and NerveTrack (Samsung), which applies a bounding box around the median and ulnar nerves when scanning the forearm.
We have more questions than answers: how does the algorithm perform across a broader range of the population? Individuals with anatomic variations? Challenges with positioning such as muscle contractures and surgical dressings? How much it will impact patient outcomes. There are potential technical limitations such as lag time, reproducibility, how artifact is handled and how the software processes images after hydrodissection, infiltration with local anesthesia or after introduction of air to the tissue planes. This study used only two adult models with normal anatomy so we do not know how the device would perform on children, women, patients at the extremes of body mass index, and those with atypical anatomy. Many anesthesiologists with a regional interest will already feel confident in blocking most patients, and therefore may only see value in this device if it could help with patients who present challenging or variant anatomy. Regional experts may be concerned that the device will encourage under-experienced practitioners to attempt PNBs beyond their skill level, and that this could lead to an increase in complications. Proponents would counter that the device may reduce the learning curve for individuals to achieve expert skill in the placement of PNBs. However, even experienced eyes may fall foul of confirmation bias by placing too much emphasis on the technology, failing to recognize false positives or false negative highlighting, especially when small or variant structures are present.
Readers may recognize many of these questions and concerns from the original introduction of ultrasound guidance to regional anesthesia. Ultrasound-guided regional anesthesia has since become the gold standard for PNB and has opened up new block techniques that would have been difficult, dangerous, or impossible using landmark-based or nerve stimulation techniques. Only time will tell if AI-guided ultrasound imaging will become the next generation gold standard for regional anesthesia safety or remains simply an expensive toy for innovators and early adopters.
References:
1. Bowness JS, Burckett-St Laurent D, Hernandez N, et al. Assistive artificial intelligence for ultrasound image interpretation in regional anaesthesia: an external validation study. British journal of anaesthesia. Feb 2023;130(2):217-225. doi:10.1016/j.bja.2022.06.031
2. Bowness JS, El-Boghdadly K, Woodworth G, Noble JA, Higham H, Burckett-St Laurent D. Exploring the utility of assistive artificial intelligence for ultrasound scanning in regional anesthesia. Regional anesthesia and pain medicine. Jun 2022;47(6):375-379. doi:10.1136/rapm-2021-103368
3. Bowness JS, Macfarlane AJR, Burckett-St Laurent D, et al. Evaluation of the impact of assistive artificial intelligence on ultrasound scanning for regional anaesthesia. British journal of anaesthesia. Feb 2023;130(2):226-233. doi:10.1016/j.bja.2022.07.049
4. Lonsdale H, Jalali A, Gálvez JA, Ahumada LM, Simpao AF. Artificial Intelligence in Anesthesiology: Hype, Hope, and Hurdles. Anesthesia & Analgesia. 2020;130(5):1111-1113. doi:10.1213/ane.0000000000004751
5. Lonsdale H, Jalali A, Ahumada L, Matava C. Machine learning and artificial intelligence in pediatric research: current state, future prospects, and examples in perioperative and critical care. The Journal of Pediatrics. 2020;221:S3-S10.
6. Antel R, Sahlas E, Gore G, Ingelmo P. Use of artificial intelligence in paediatric anaesthesia: a systematic review. BJA Open. 2023;5:100125.