
Arterial lines - Could we do less and still achieve the same outcomes?
Matthew J Rowland, MD, Ethan Sanford MD, Shawn Jackson MD PhD

Three pediatric anesthesiologists walk into a bar… five minutes later, every patron has an arterial line. You know, just in case.
We love arterial lines. Today’s PAAD was a shot through the heart. Arterial lines have numerous indications and uses in the OR and ICU. Continuous blood pressure monitoring may improve quantification of the intensity and duration of abnormal physiology. New waveform metrics allow SVR and pulse pressure variation estimation, which may improve clinical decision making. Arterial lines also allow lab measurements and provide better information on pH, oxygenation, CO2 clearance and hemoglobin.1 However, individual and institutional variance in arterial line deployment exists, just as a national survey of pediatric ICU doctors showed wide variation in arterial line placement for certain disease states.2 But the big question is, do arterial lines really help us take better care of patients? Today’s PAAD looks to an interesting randomized control trial in adult ICU patients that challenges the assumption that arterial lines improve outcomes.
Original Article
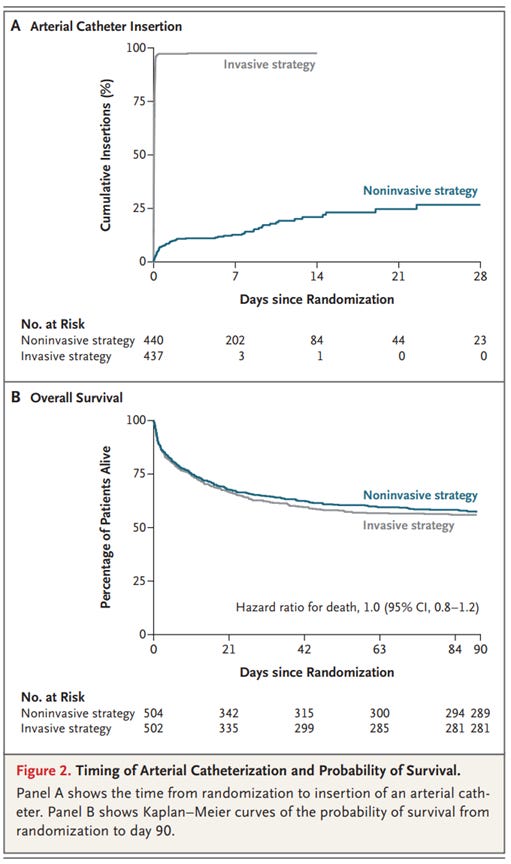
Muller G, Contou D, Ehrmann S, Martin M, Andreu P, Kamel T, Boissier F, Azais MA, Monnier A, Vimeux S, Chenal A, Nay MA, Salmon Gandonnière C, Lascarrou JB, Roudaut JB, Plantefève G, Giraudeau B, Lakhal K, Tavernier E, Boulain T; CRICS-TRIGGERSEP F-CRIN Network and the EVERDAC Trial Group. Deferring Arterial Catheterization in Critically Ill Patients with Shock. N Engl J Med. 2025 Nov 13;393(19):1875-1888. doi: 10.1056/NEJMoa2502136. Epub 2025 Oct 29. PMID: 41159885.
Muller et al. randomized 1010 adult patients with sepsis to a non-invasive strategy (no arterial line) and an invasive strategy (arterial line placement). Twenty-eight day any cause mortality was the primary outcome. For patients with an arterial line placed, the mortality rate was 36.9%, and for those without an arterial line the mortality rate was 34.3%, not meeting prespecified thresholds for statistical significant differences. Now, 25% of patients in the non-invasive group did eventually get arterial lines placed, though often much later than the invasive group.
So what does this mean? Arterial lines, similar to the old Swan-Ganz catheters, have never been shown to improve patient outcomes.3,4 So are we overusing arterial lines in pediatrics? Will they meet the same fate as PA lines?
Well first, a few caveats. This study’s main outcome is mortality, which is relatively high in this population, but much less applicable to pediatric anesthesia. We don’t tie our shoes because we might die if we don’t, but it makes wearing shoes easier. Similarly, while arterial lines may make the job of keeping children safe easier, measuring that difference may prove difficult. Second, interestingly enough, there was actually more pain or discomfort in the non-invaive group (13.1%) due to frequent blood pressure cuff cycling compared to the invasive group (9%) and this difference was significant. Third, patients in the non-invasive group still required arterial puncture procedures for blood gas analysis, subjecting these patients to significantly more arterial puncture attempts (742) compared ot the invasive monitoring group (269). This study also doesn’t capture important outcomes such as kidney injury or cerebral injury that may be different between the groups due to more tight blood pressure control. Additionally, although vasopressor usage was similar between the groups, time within a target blood pressure is not well represented in the groups. Furthermore, the study population of sick adult ICU patients is fundamentally different from a child undergoing surgery who may or may not become unstable during the episode of care when arterial lines may aid in recognition and more nuaned resuscitation. Finally, the risks of arterial lines should also be considered. Peripheral arterial lines have low rates of infection, vascular compromise, or nerve injury.5 These risks are likely to diminish in the modern era of ultrasound and are radically different from the risks of PA catheters.
What are your thoughts and practices regarding arterial line placement? How have your practice patterns changed since training and over time? Send your thoughts to Myron (myasterster@gmail.com) and he will post in a Friday reader response.
References
1. Biais M, Ehrmann S, Mari A, et al. Clinical relevance of pulse pressure variations for predicting fluid responsiveness in mechanically ventilated intensive care unit patients: the grey zone approach. Crit Care. 2014;18(6):587. Published 2014 Nov 4. doi:10.1186/s13054-014-0587-9
2. Pilarz MS, Mattson CD, Pritchett CM, Rountree AK, Rowland MJ. Practice Variation in Arterial Catheter Placement: A Survey of Pediatric Critical Care Practitioners. J Intensive Care Med. Published online September 1, 2025. doi:10.1177/08850666251363551
3. Gershengorn HB, Wunsch H, Scales DC, Zarychanski R, Rubenfeld G, Garland A. Association between arterial catheter use and hospital mortality in intensive care units. JAMA Intern Med. 2014;174(11):1746-1754. doi:10.1001/jamainternmed.2014.3297
4. Sionis A, Rivas-Lasarte M, Mebazaa A, et al. Current Use and Impact on 30-Day Mortality of Pulmonary Artery Catheter in Cardiogenic Shock Patients: Results From the CardShock Study. J Intensive Care Med. 2020;35(12):1426-1433. doi:10.1177/0885066619828959
5. Gleich SJ, Wong AV, Handlogten KS, Thum DE, Nemergut ME. Major Short-term Complications of Arterial Cannulation for Monitoring in Children. Anesthesiology. 2021;134(1):26-34. doi:10.1097/ALN.0000000000003594
Anecdotally I’ll have the cliché comment of “I’ve never regretted putting in that art-line”. But it rings true for me. The shoelace metaphor was bang on! Thank you for sharing.