
Adding acetaminophen (paracetamol) or hydromorphone to ibuprofen did not improve analgesia in pediatric musculoskeletal pain after minor injuries
Myron Yaster MD, Rita Agarwal MD FAAP, Elliott Krane MD and Lynne G. Maxwell MD FAAP

In today’s PAAD, Ali et al. [1] in a randomized controlled double masked (“blind”) study, investigated the effects of adding an oral opioid (hydromorphone 0.05 mg/kg) or acetaminophen (15 mg/kg) to ibuprofen given alone or in combination in outpatient, pediatric musculoskeletal pain management. As the authors themselves clearly state: “The trial has several limitations. First, only children with nonoperative injuries were included. Therefore, results may not be applicable to postoperative settings.”[1]
So why review it in the PAAD? This is a very large study (8098 children were screened for eligibility; 699 were randomized and 653 were included in the efficacy analyses), and it is well designed and executed. But this study does not confirm that opioids are unnecessary for surgical and postoperative analgesia, although we know that in some procedures NSAIDs and acetaminophen may be used without opioids. [2, 3] Therefore this paper should not be construed to mean that opioids are unnecessary in orthopedic surgery although a casual reader of the title and abstract alone may conclude this. Myron Yaster MD
Original article
Ali S, Klassen TP, Candelaria P, Bhatt M, Sawyer S, Stang A, Yaskina M, Heath A, Pechlivanoglou P, Offringa M, Drendel AL, Hickes S, Poonai N; KidsCAN PERC Innovative Pediatric Clinical Trials No OUCH Study Team. Acetaminophen (Paracetamol) or Opioid Analgesia Added to Ibuprofen for Children’s Musculoskeletal Injury: Two Randomized Clinical Trials. JAMA. 2026 Jan 8:e2525033. doi: 10.1001/jama.2025.25033. Epub ahead of print. PMID: 41505155; PMCID: PMC12784265.
The objective of today’s PAAD was “To determine in children with musculoskeletal pain whether treatment with an opioid (hydromorphone) plus ibuprofen or nonopioid (acetaminophen [paracetamol]) plus ibuprofen decreased pain scores compared with ibuprofen alone.”
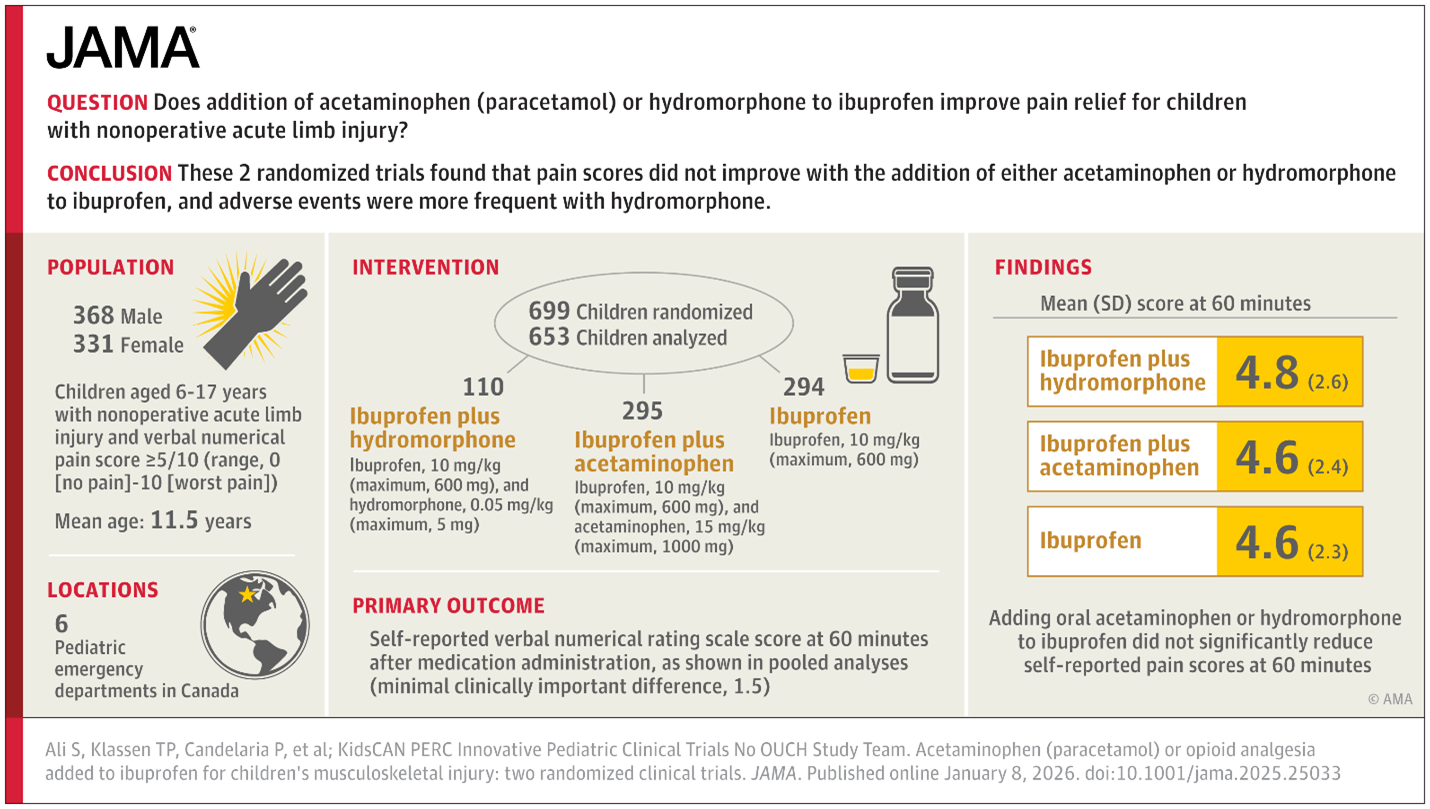
The opioid trial randomized participants to a single oral dose of ibuprofen plus hydromorphone, plus acetaminophen, or to ibuprofen alone. The nonopioid trial randomized participants to a single oral dose of ibuprofen plus acetaminophen or ibuprofen alone. In all groups, ibuprofen was dosed at 10 mg/kg (maximum, 600 mg). The acetaminophen dose was 15 mg/kg (maximum, 1000 mg), and the hydromorphone dose was 0.05 mg/kg (maximum, 5 mg). The primary efficacy outcome was self-reported vNRS pain score at 60 minutes post medication administration (score range, 0 [no pain] to 10 [worst pain]; with a defined minimal clinically important difference of 1.5). The primary safety end point was the proportion of children with any adverse event related to study drug administration.”[1]
What did they find? “The mean (SD) age of children in the 2 trials was 11.5 (+/- 3.5) years and about half were female. The mean (SD) vNRS score at recruitment was 6.4 (1.8). In pooled analyses, mean (SD) vNRS scores 60 minutes after drug administration were 4.8 (2.6) in the ibuprofen plus hydromorphone group, 4.6 (2.4) in the ibuprofen plus acetaminophen group, and 4.6 (2.3) in the ibuprofen alone group (clearly no significant differences). Adverse events occurred at higher rates in the ibuprofen plus hydromorphone group (28.2%) compared with the ibuprofen plus acetaminophen (6.1%) or ibuprofen alone groups (5.8%). No serious adverse events occurred.”[1]
Simply stated: there wasn’t an added benefit of adding oral acetaminophen or hydromorphone to ibuprofen in non-operative musculoskeletal pain. The analgesic effects of NSAIDs in this study appear to provide adequate analgesia for musculoskeletal pain.
But what is “musculoskeletal pain” as defined in this study? The majority were injuries that occurred to the upper extremity (wrist, fingers, forearm) with the mechanism of injury primarily being slips, trips, falls or team sports injuries. Over half were “bruises” and fewer than a third were fractures, including finger, toe and wrist fractures. Only 9 out of 700 patients had bike/scooter/skateboard injuries and no injuries resulted from bike or motor vehicle collisions, while almost the rest were from falls, trips , athletic or “other play.” In other words, these were bread and butter minor childhood and teenage injuries, the majority of which would ordinarily NOT be treated with opioids in emergency departments as far as one can tell.
The results of this study are hardly surprising. Mechanistically the addition of acetaminophen or hydromorphone might improve analgesia, but not much if adequate analgesia was produced by an NSAID in the setting of minor orthopedic injuries, i.e. sprains and contusions. And acetaminophen effect might be expected to be overshadowed by the NSAID when given simultaneously. For anesthesiologists, this study adds little to what is already practiced and has no relevance to providing postoperative analgesia to surgical orthopedic patients. How can the ED treatment of minor bruises and sprains apply to bone cutting and spine straightening?
Send your thoughts and comments to Myron (myasterster@gmail.com) and he will post in a Friday reader response.
References
1. Ali S, Klassen TP, Candelaria P, Bhatt M, Sawyer S, Stang A, Yaskina M, Heath A, Pechlivanoglou P, Offringa M et al: Acetaminophen (Paracetamol) or Opioid Analgesia Added to Ibuprofen for Children’s Musculoskeletal Injury: Two Randomized Clinical Trials. Jama 2026.
2. Hansen EE, Chiem JL, Low DK, Rampersad SE, Martin LD: Enhancing Outcomes in Clinical Practice: Lessons Learned in the Quality Improvement Trenches. Anesthesia and analgesia 2024.
3. Chiem JL, Franz AM, Hansen EE, Verma ST, Stanzione TF, Bezzo LK, Richards MJ, Parikh SR, Dahl JP, Low DK et al: Optimizing pediatric tonsillectomy outcomes with an opioid sparing anesthesia protocol: Learning and continuously improving with real-world data. Paediatric anaesthesia 2024, 34(11):1087–1094.